HyperArc - How Many Targets are Possible?
Since we are the only HyperArc center in Austria, we are often asked: "What is the maximum number of lesions that you can treat simultaneously?" This will be today's topic.
Lesions and Targets
First we have to clarify the terminology. The Treatment Planning System (TPS) for HyperArc is Eclipse (we currently use 18.1). In Eclipse, each Structure that should receive a certain minimum dose is called a Target Structure, or simply Target. Clinicians on the other hand speak of Lesions. If, for instance, a patient has, say, five Brain Metastases (BMs) that should be irradiated, there are five lesions to treat.
Using the well known margin concept, each lesion consists of three overlapping structures: the Gross Tumor Volume (GTV), the Clinical Target Volume (CTV), and the Planning Target Volume (PTV). In HyperArc planning, we contour the GTV on the planning CT (plus registered MR information). From the GTV, we create the CTV by adding an isotropic margin of 1 mm, and the PTV out of the CTV by adding 2 mm. This means that the GTV-to-PTV margin is 3 mm. This is done for all lesions.
As described in the previous article on HyperArc, the desired dose distribution in each lesion has the prescription dose at the PTVs outer border, and increases towards center. In our department, the innermost structure, the GTV, should get the Center Dose. The dose distribution inside the GTV should be homogeneous, which means that all voxels inside the GTV should receive the same dose1. A typical Dose Prescription would be: all lesions should receive 6 Gy at the border and 7.5 Gy in the center in five fractions, which means that the Total Prescribed Dose is 30 Gy, and center dose is 37.5 Gy.
Next step is to convert Lesions into Targets. According to Varian, the Photon Optimizer (PO) of Eclipse works best with non-overlapping structures. Since PTV/CTV/GTV still are overlapping, we segment them by forming non-overlapping, onion-like shells. In VMAT Optimization, each shell will be a separate Target. If we use the PTV-CTV shell, the CTV-GTV shell and the GTV as Targets, we get three Targets per Lesion2. The title of the previous article is therefore somewhat click-bait, because it spoke of "45 targets", which could be falsely interpreted as "45 lesions".
Now that we have clarified the terminology, we come back to today's topic. The idea is to use a clinical case, add some more (non-clinical) lesions, create the new targets, perform PO optimization, calculate dose, and repeat the cycle until something either fails in Eclipse or the process becomes so slow that it unpractical to proceed. Since both RAM and GPU memory are limited (both PO optimization and AXB dose calculation use the GPU), there must be a practical limit.
We do not expect a "hard limit" valid for all patients, because memory consumption depends on the individual patient data set (number of slices, grid and voxel sizes, optimization settings etc).
We start by describing the start conditions in the clinical (treated) plan.
Start Conditions
The patient has seven lesions which shall receive identical fraction dose (9 Gy at the border and 11.25 Gy at the center) in three fractions. Total prescribed dose is 27 Gy, with 33.75 Gy center dose.
The CT dataset has 299 slices (1 mm slice thickness), and the lateral pixel size is 0.6 mm x 0.6 mm. Based on CARE kV, the scanner selected 80 kV for the scan. Dose will be calculated on this 80 kV scan.
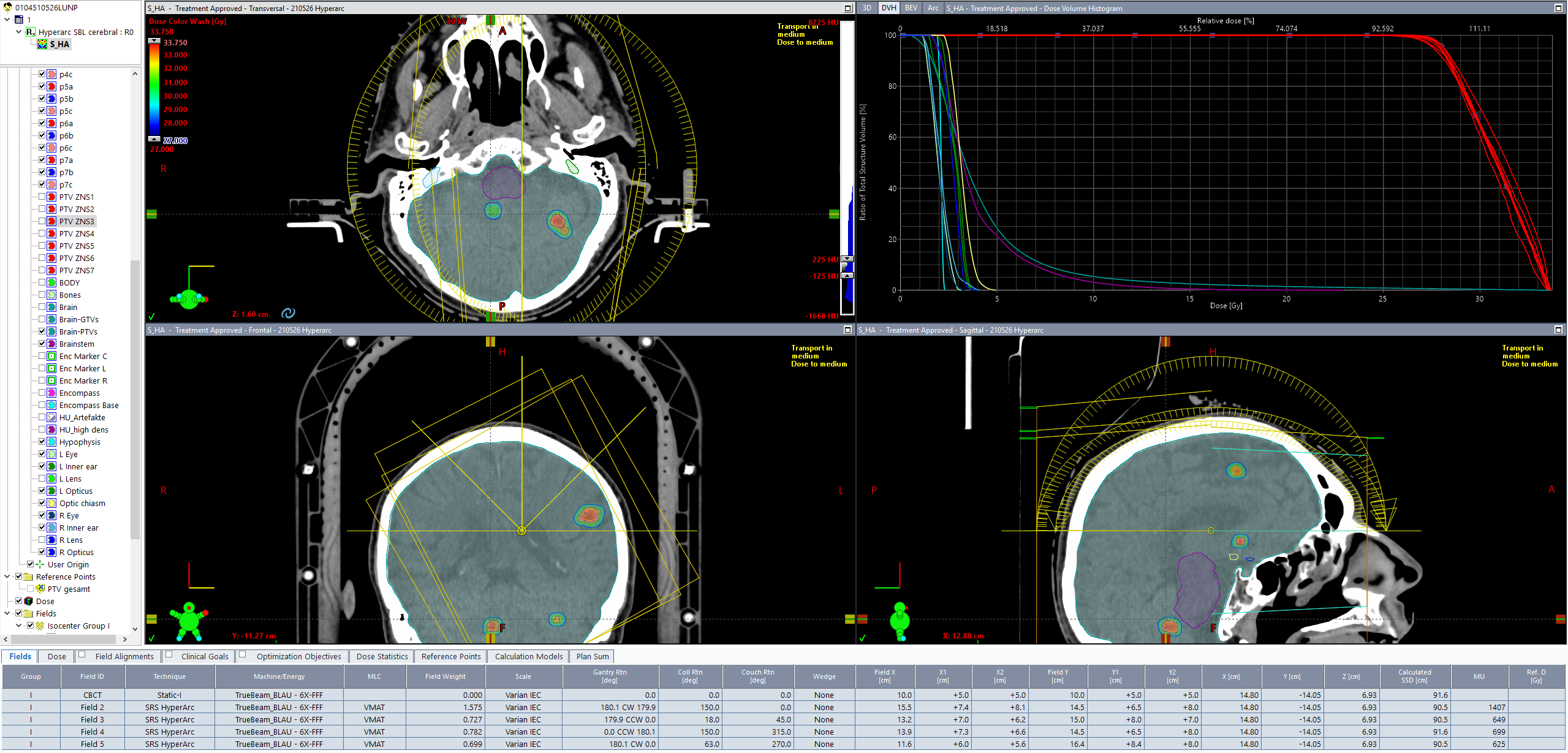
Because the seven lesions are distributed rather evenly within the brain, the HyperArc module calculated a central isocenter location. All four arcs, with couch angles 0°, 45°, 315° and 270° are activated by the software:
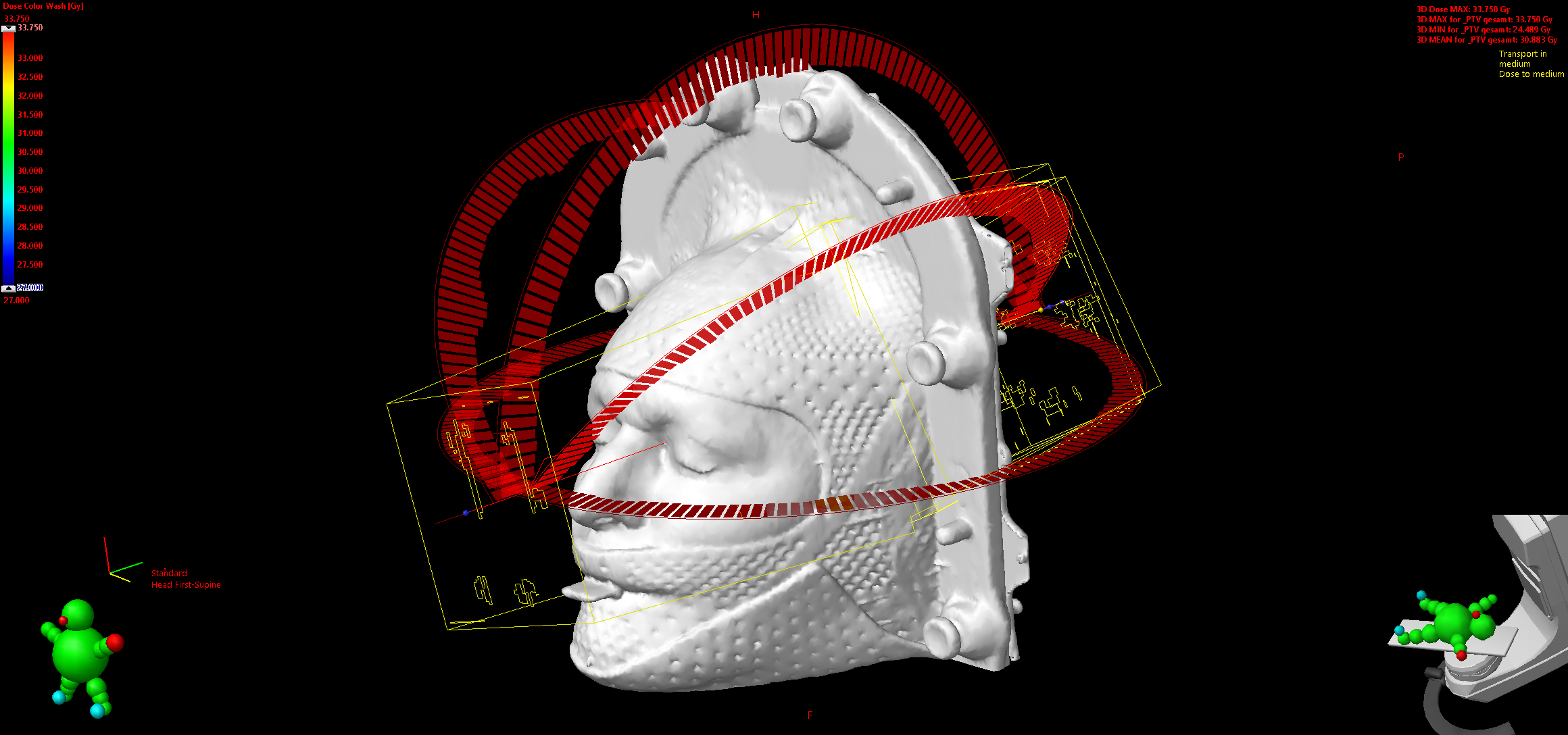
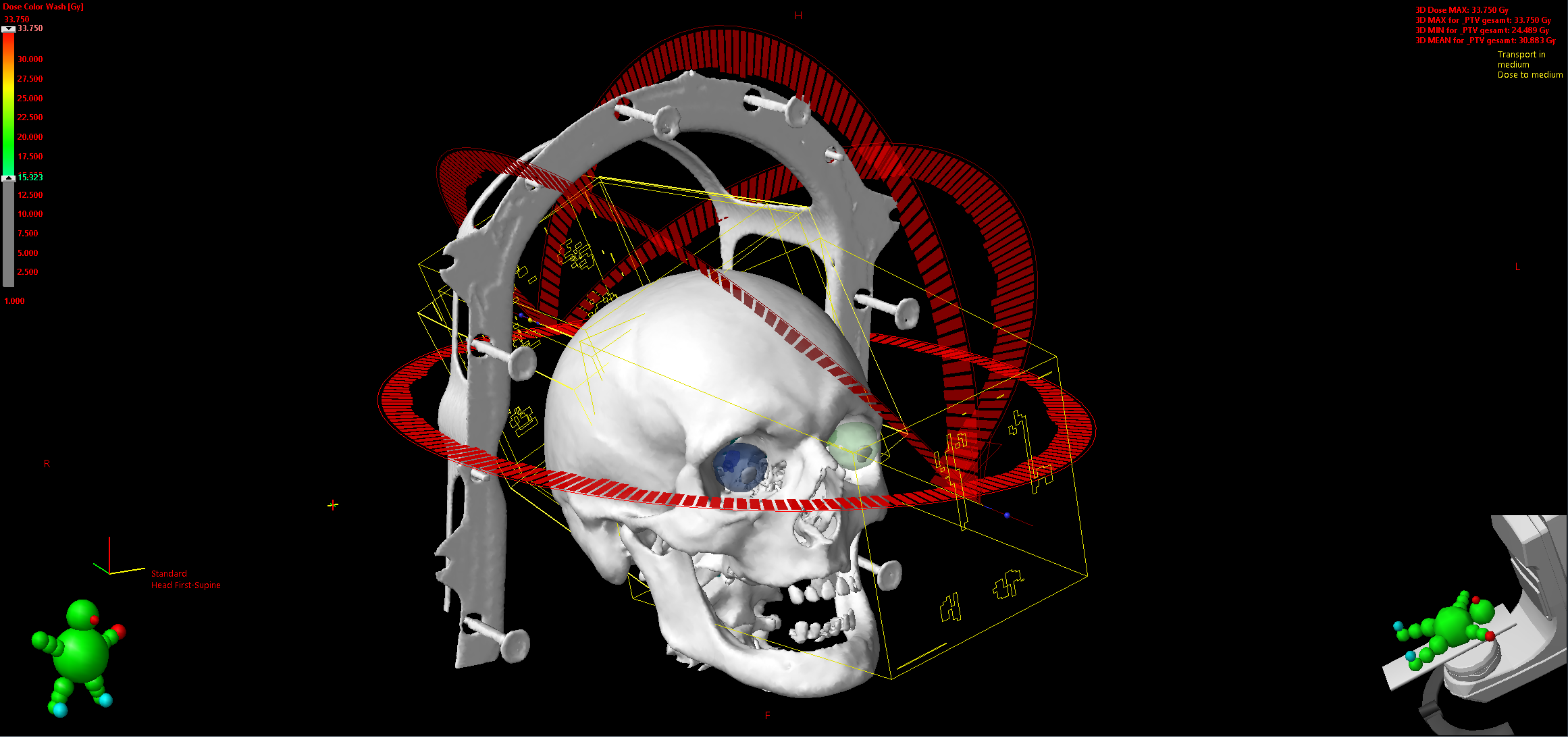
(Field arrangement of the clinical HyperArc case, two different views, "Normal" and "Halloween" ;-)
When we received the case for planning, GTV/CTV/PTV were already contoured. We started by defining the several non-overlapping target shells and some other structures such as Brain-GTV, which are used to evaluate the clinical goals (Timmerman tables). It took 30 minutes until all structures were ready and the the actual optimization could start. The first acceptable plan was ready after another 35 minutes. This is fast, considering that all resolution settings were set to "High" or "Fine" (PO dose calculation resolution, Structure resolution) and the calculation grid size was set to 1 mm.
A good HyperArc plan can be created within an hour or so, but of course, one tries to optimize further, creating more plan variants. For this patient, the third plan was accepted for treatment3.
Adding More Targets
We now leave the clinical case by duplicating the Structure Set. To the copy, we want to add eight more lesions which have no clinical meaning and which we distribute randomly inside the brain.4 Using the 3D-brush, we draw the GTVs (about 3-4 mm diameter), generate CTVs and PTVs by adding the margins, and create the non-overlapping shells.
This gives a current total of 15 lesions:
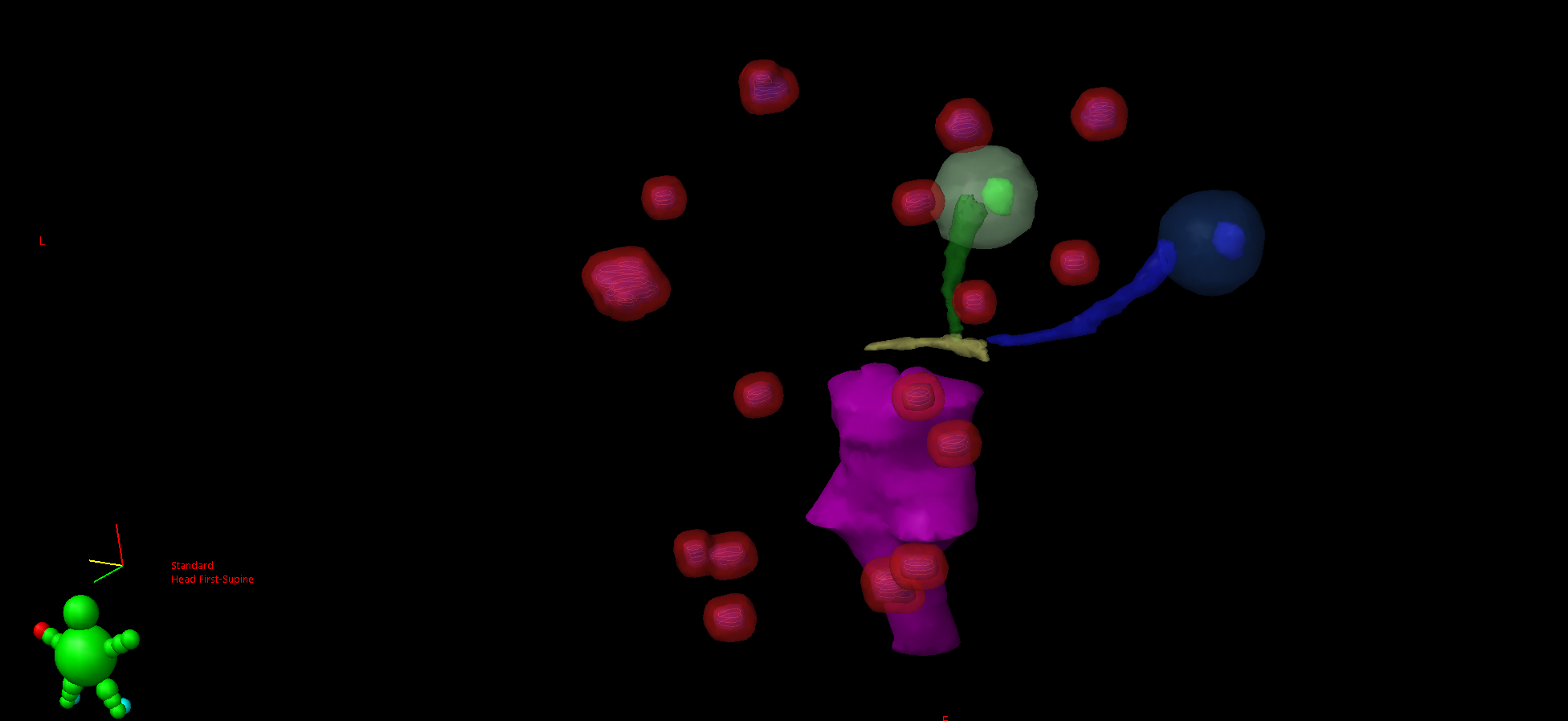
(One of the clinical lesions - lower left - is a double-lesion, which is counted as one. Eyes, brainstem and optical nerves are shown for orientation.)
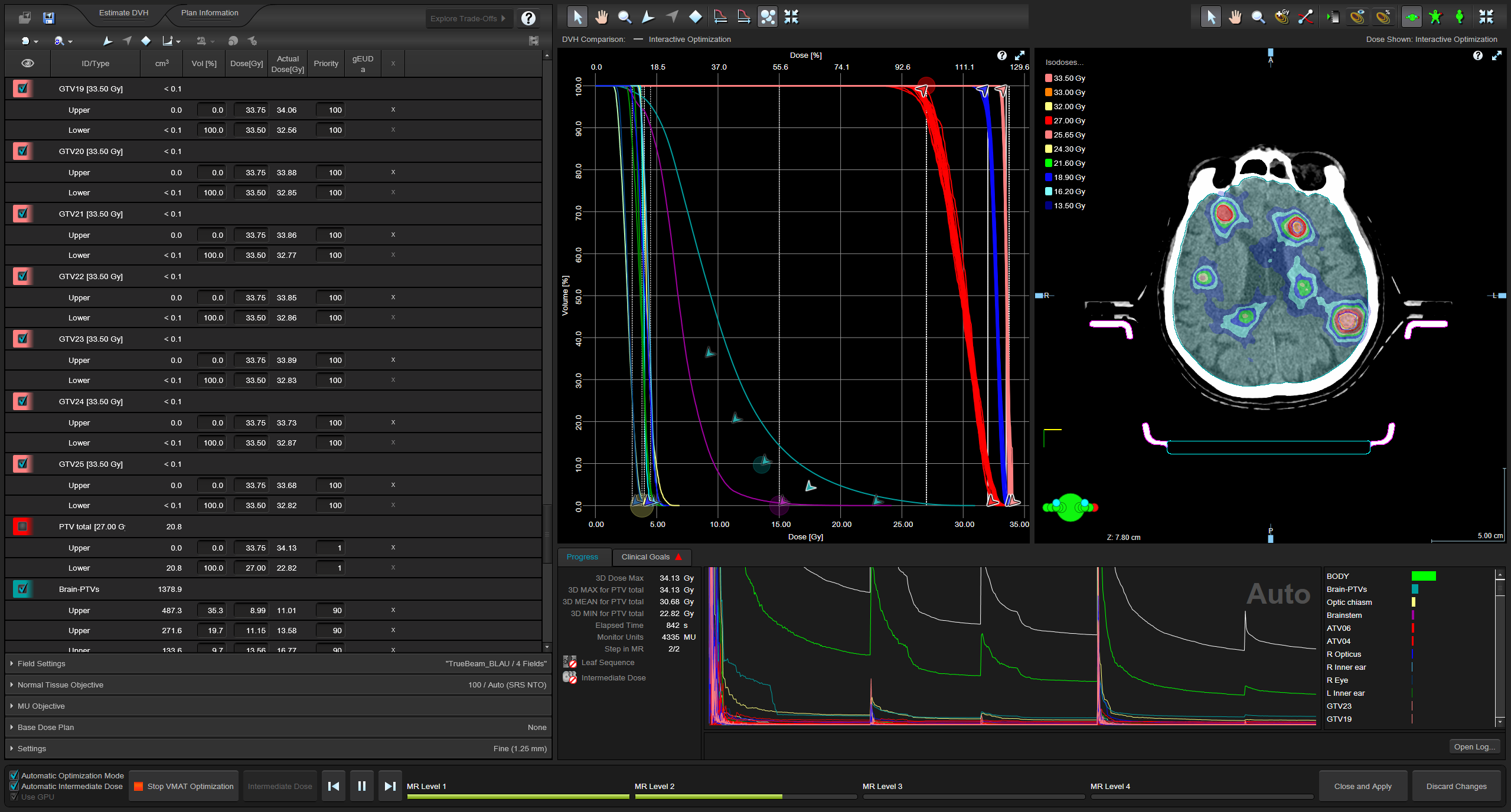
We now switch from Contouring to the Optimization window. The default Varian HyperArc workflow only generates "lower" objectives for each target. However, we prefer to use "upper" objectives as well. This means that for each of the 45 targets, an upper objective must be added, plus the desired dose level, plus the Priority for each objective. The list on the left of the PO window (yellow frame) is actually more than 6 pages long!
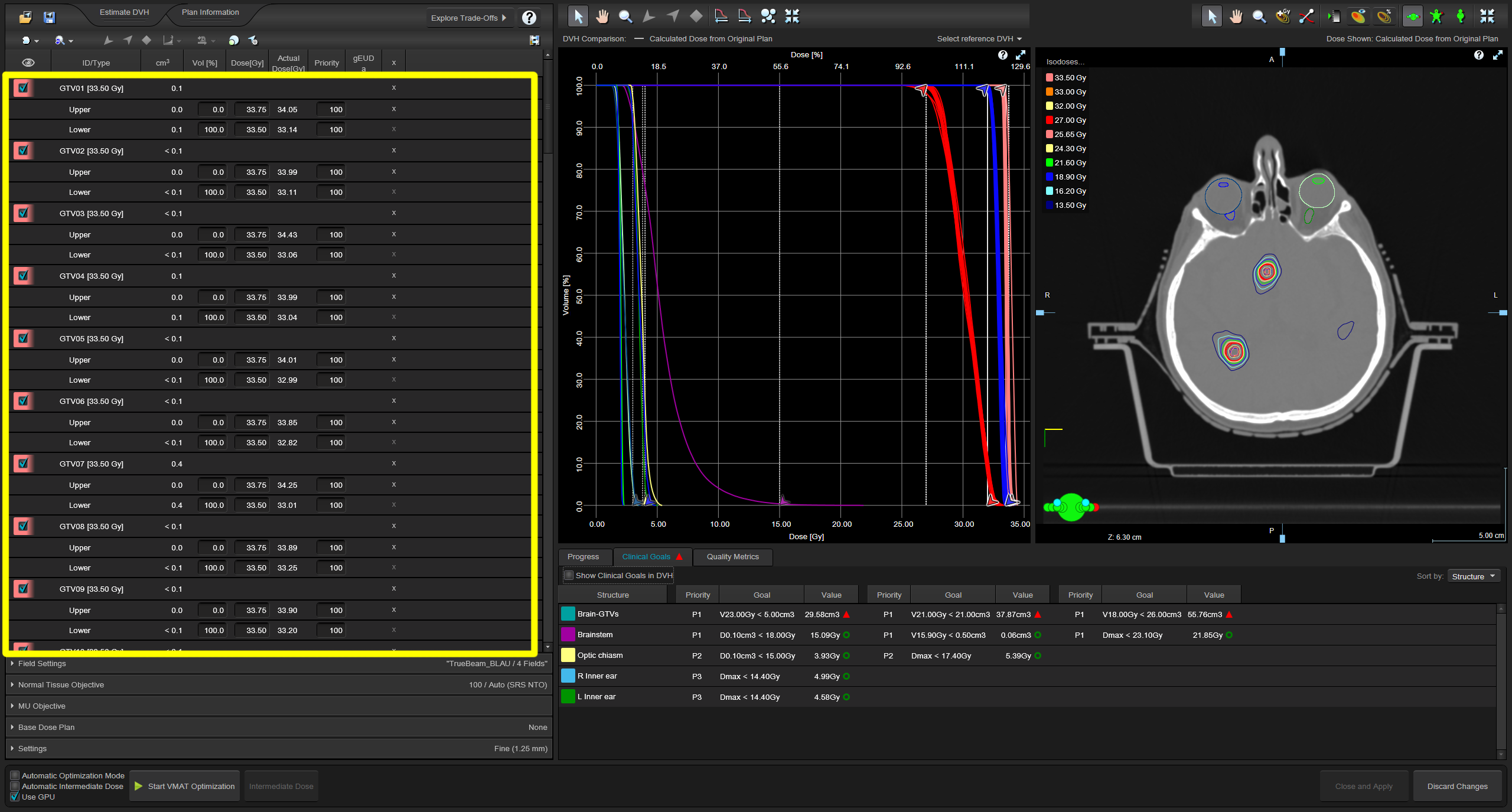
During all this adding and editing, we notice that the user interface starts to slow down. It takes considerably longer the more items are added to the list. But once the edits are finished, optimization itself still performs without issues.
Warm-Up: 20 Lesions, 61 Targets
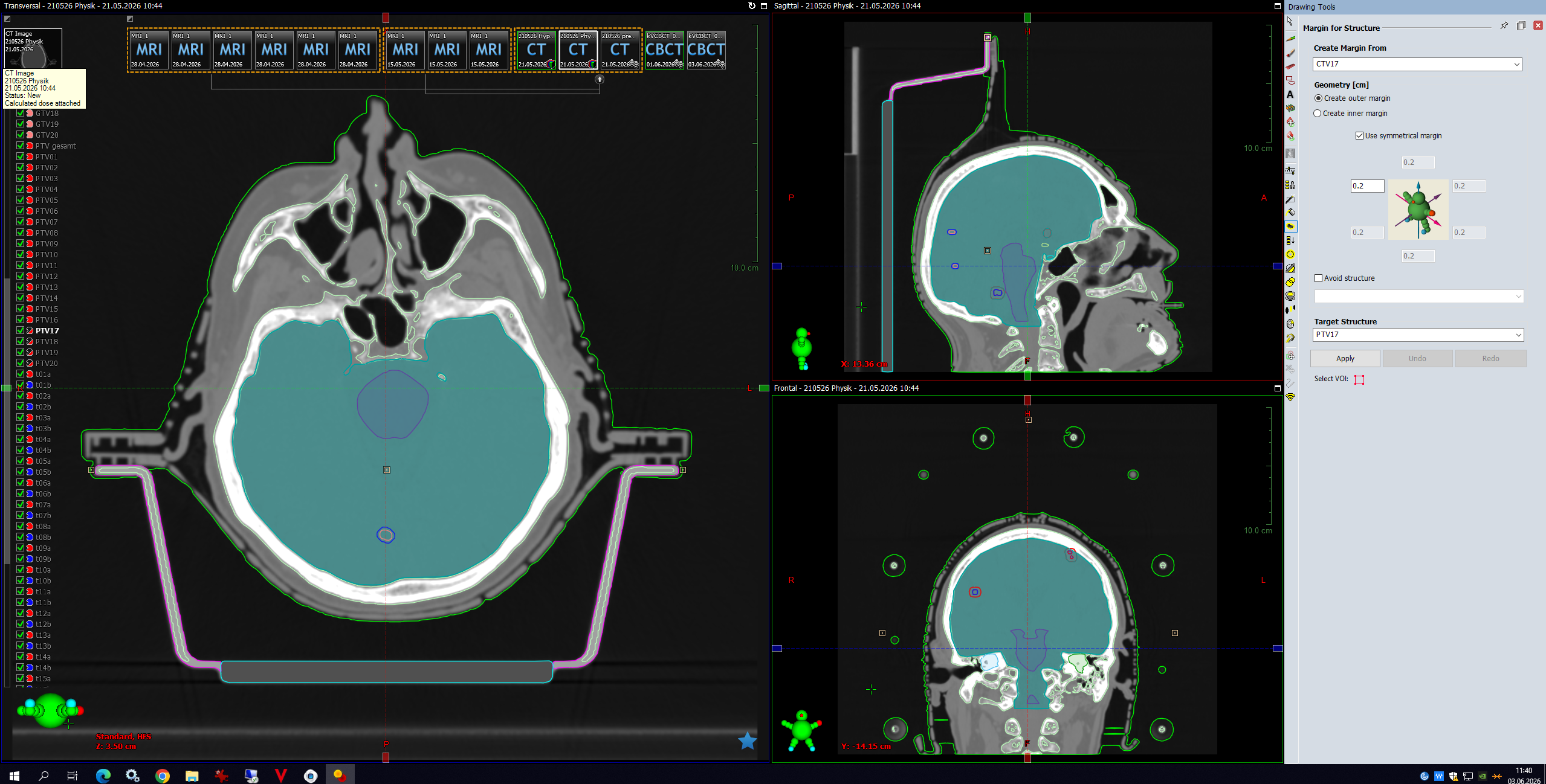
Twenty lesions means 60+ targets, and we start being cautious and save after each major editing step. This screenshot is from Contouring workspace, where we currently generate the PTV17 by adding the marging to CTV17:
While writing this text, we change our naming convention regarding the shell structures. Instead of calling them t16a and t16b, we choose ATV16 and BTV16. This has many advantages, from creating new structures (right-clicking ATV16 and selecting "Duplicate Structure" automatically creates ATV17) to alphabetic ordering: ATV20/BTV20/GTV20 are now the three non-overlapping targets for lesion 20. We repeat the renaming for all lesions and do not forget to update the Brain-GTVs, the Brain-PTVs and PTV total structures after adding more lesions.
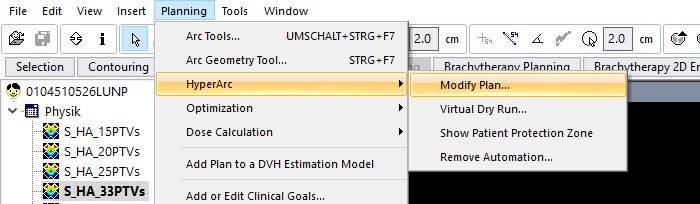
The advantages of the new naming scheme change become obvious when we select "Modify HyperArc Plan" from the menu. The "A" and "B" shell targets are nicely grouped together, which makes it easy to insert the correct prescribed doses:
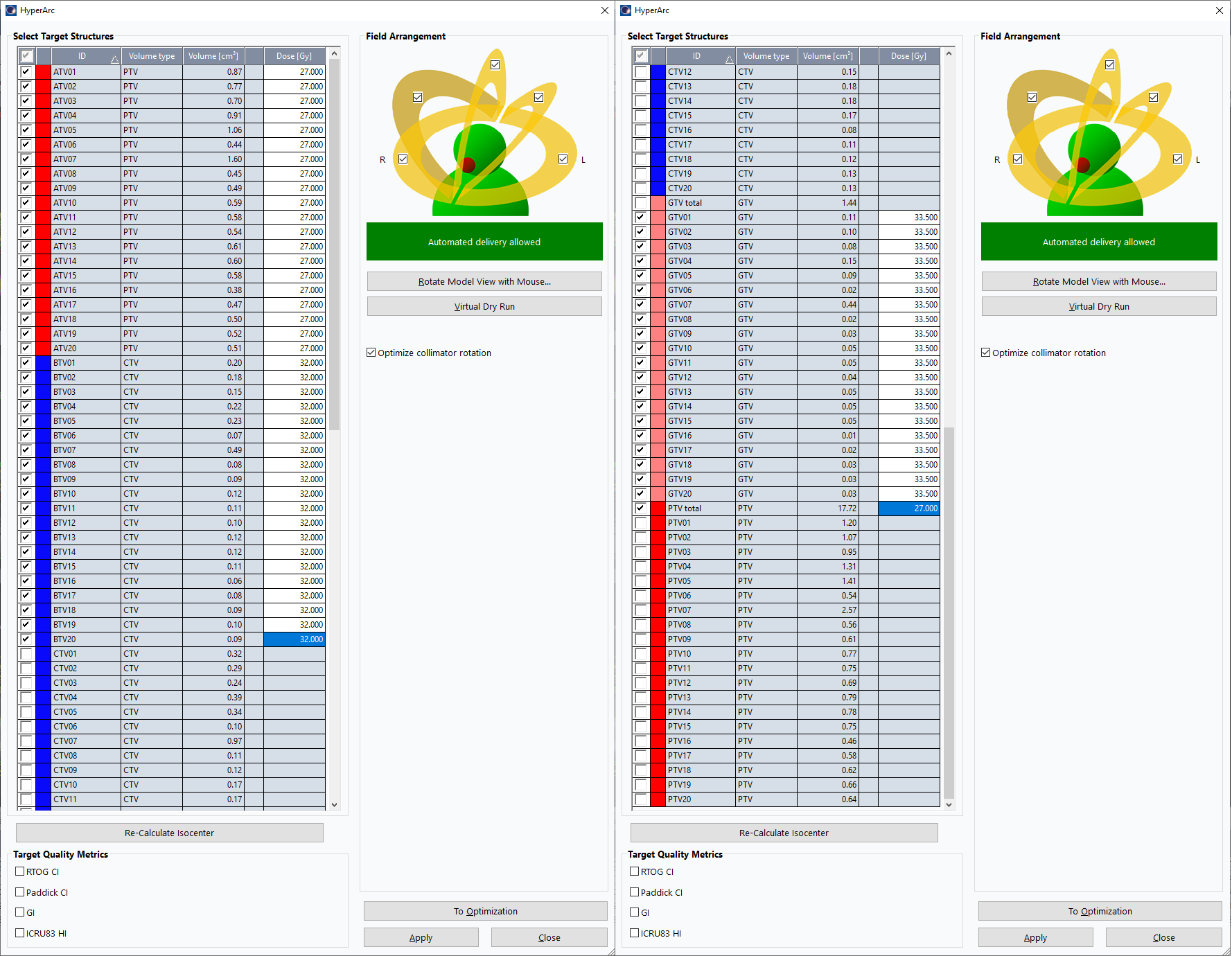
Unfortunately, since this is Varian philosophy, only the lower (prescribed) doses can be added here, not the upper limits. This has to be done in the PO Optimizer window.
After each edit in the user interface, one has to wait a few seconds until the screen is updated. With a little experience, on can click a few fields in advance and enter the values, until the UI responds.
With 20 lesions (61 targets), after clicking "Start VMAT Optimization" it took 4 minutes 25 seconds until the first iteration appeared.
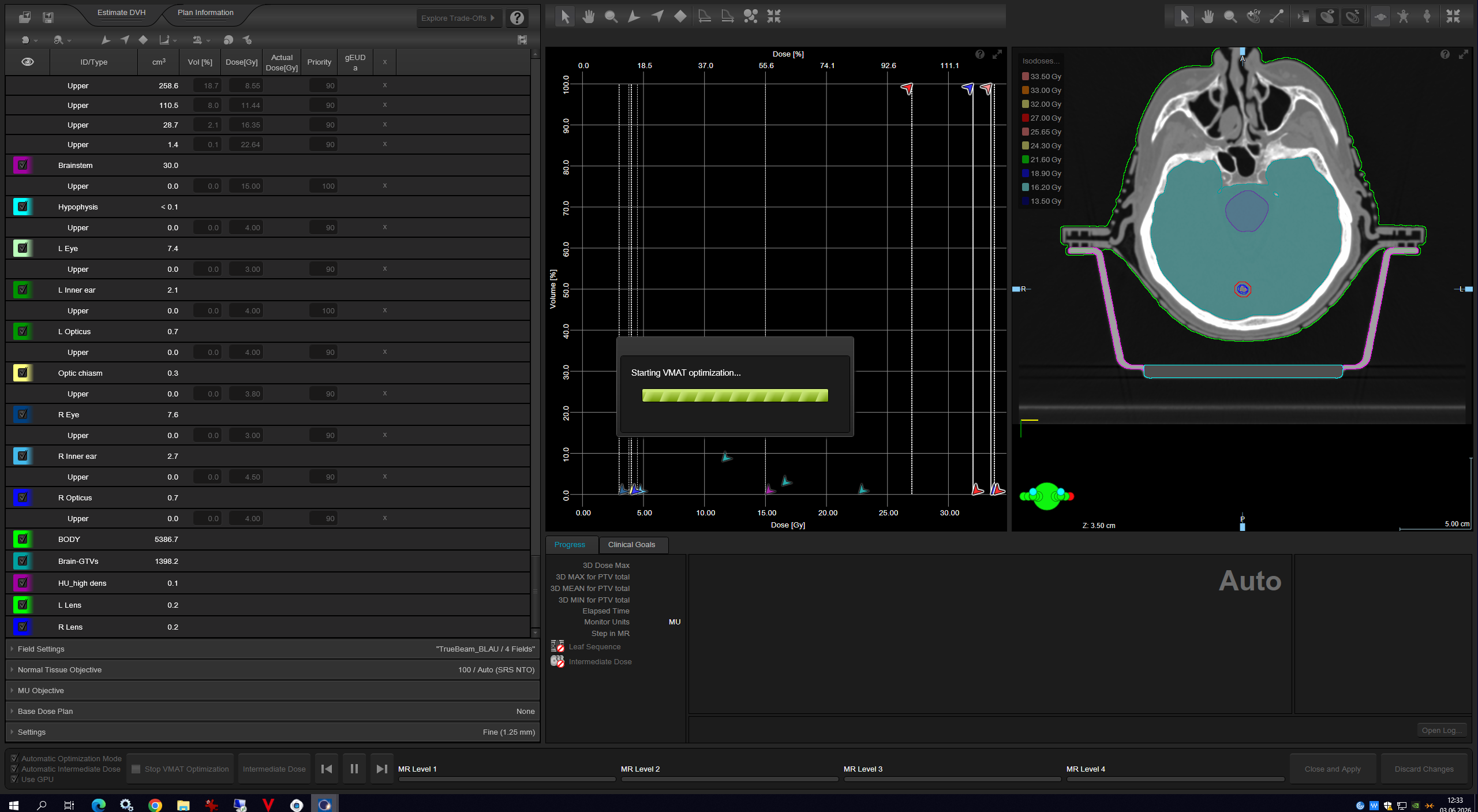{kind=link}
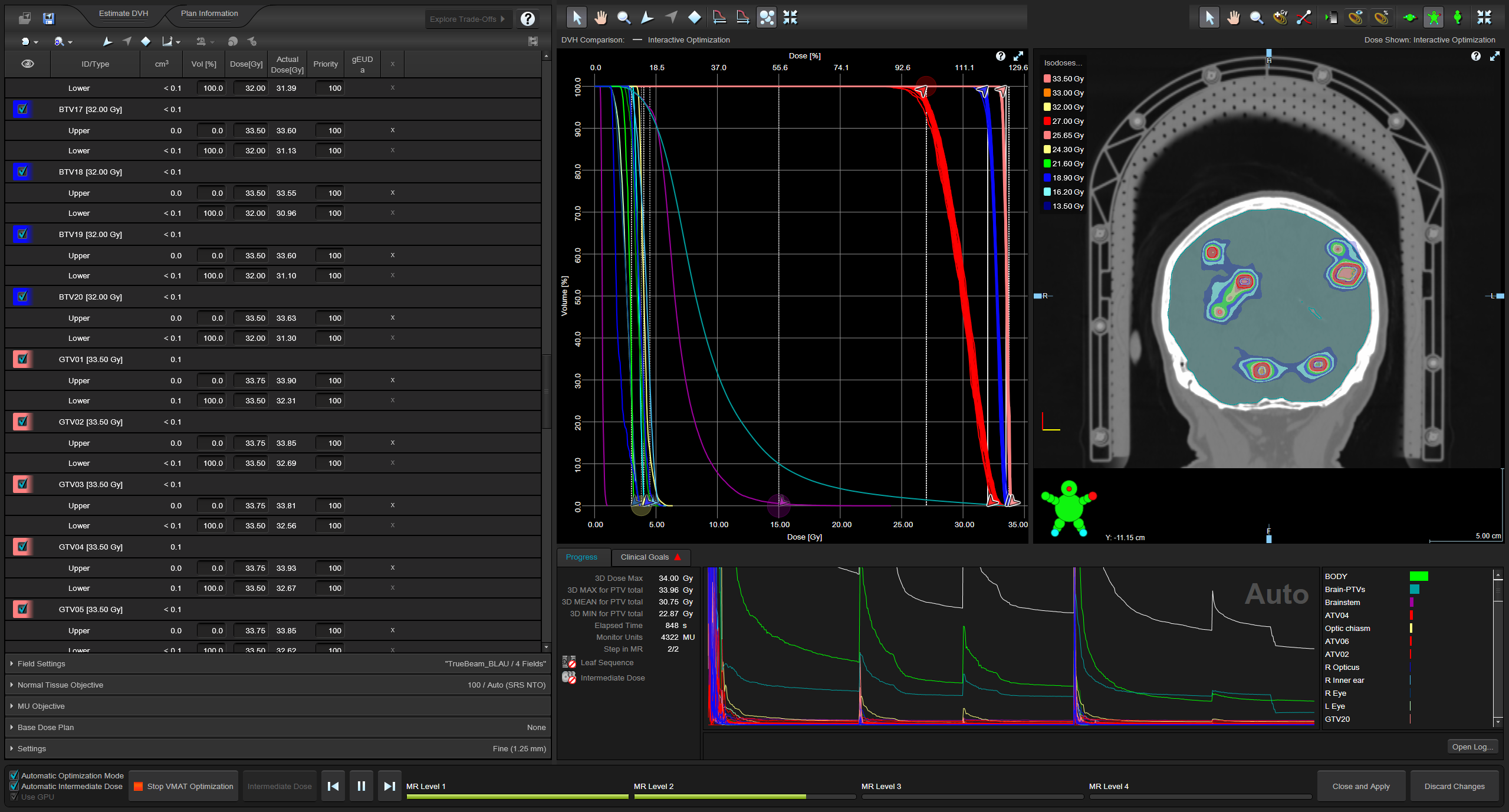
(20 lesions, 13min into GPU optimization.)
After four optimization levels (MR Level 1-4), at 27 minutes into optimization, Intermediate Dose was calculated. This took about 3 minutes. 35 minutes into optimization, we are still looking good:
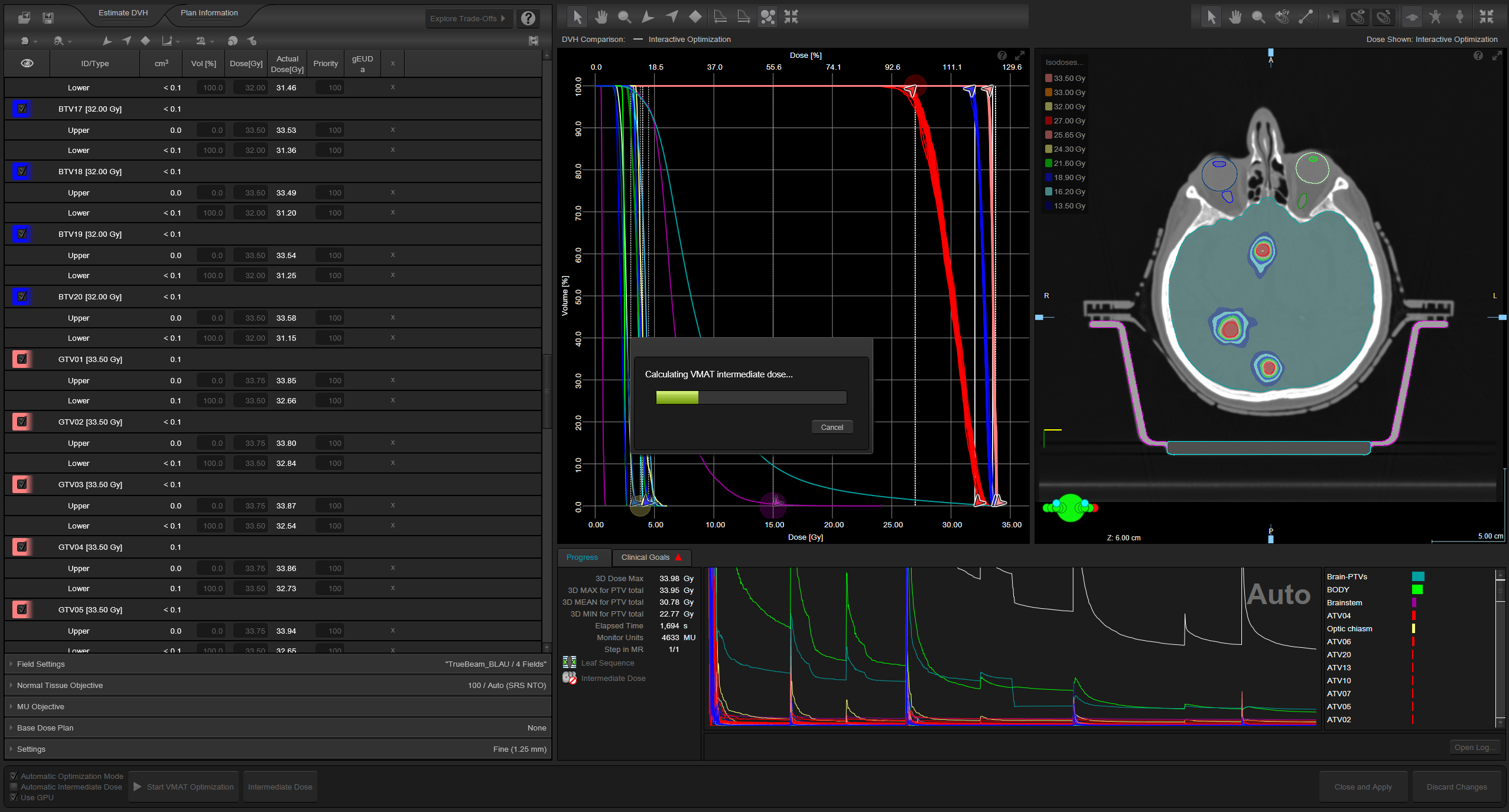{kind=link}
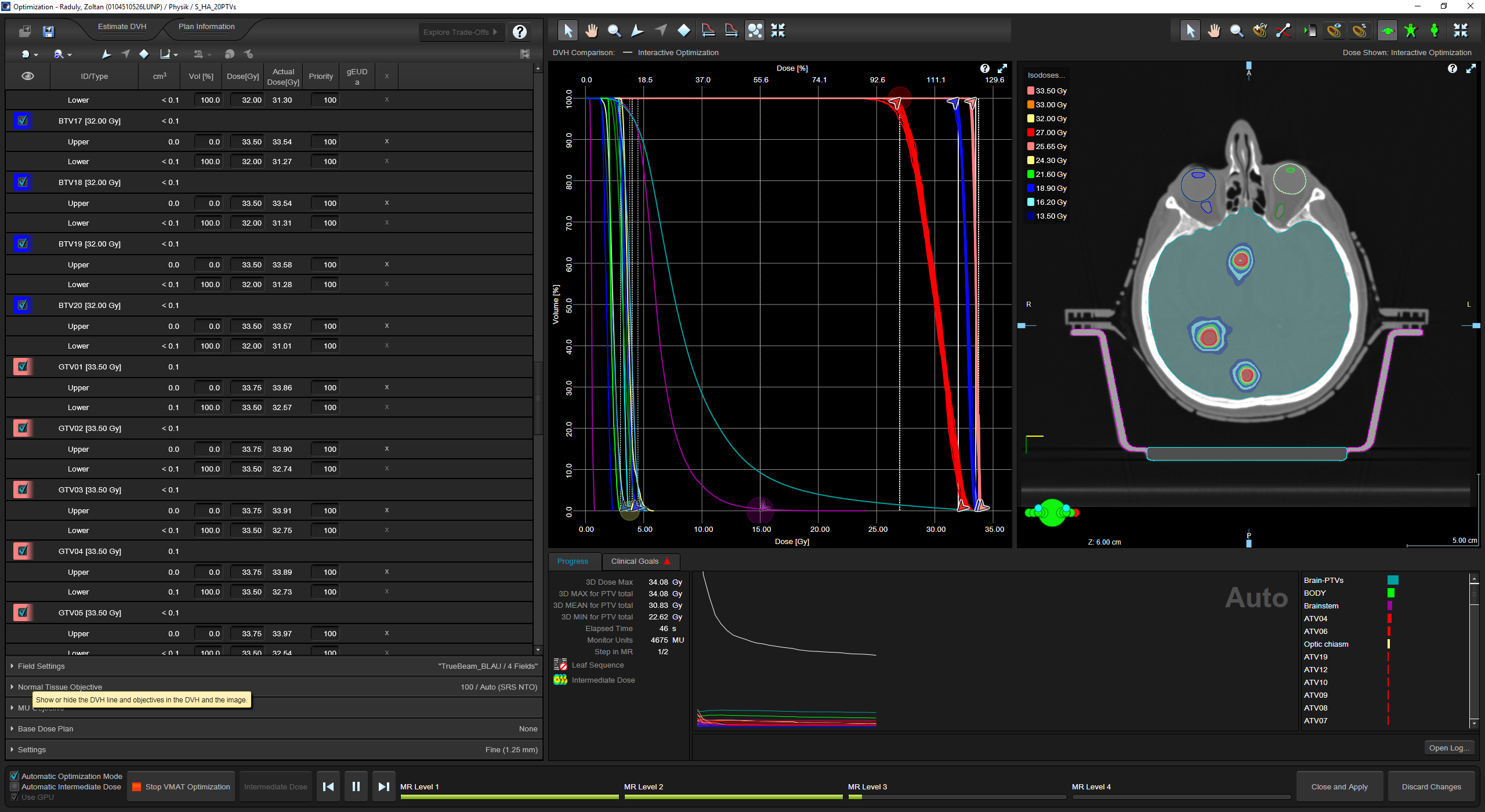
Exactly 49 min 15 sec after start of optimization, we had the final 3D-calculated plan:
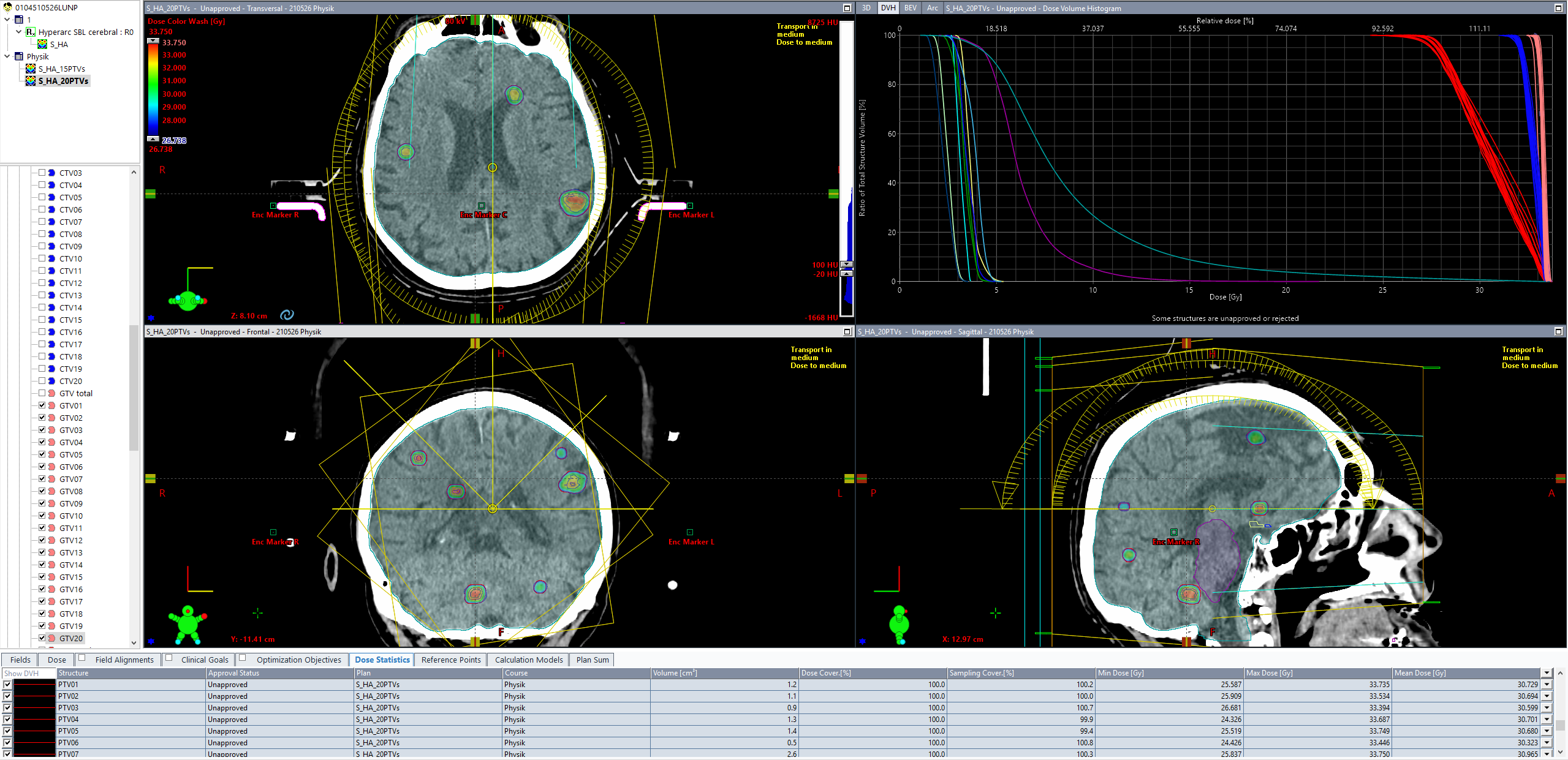
(Final dose for 20 lesions. The good image contrast in the brain is due to the 80kV scan.)
We can conclude that 20 lesions (61 targets) are still no problem, if the planner is not in a hurry.
Next Step: 25 Lesions, 76 Targets
Adding five more lesions is straightforward. In Contouring, the editing process is still fast. Adding the "Upper" objectives to the ATVs, BTVs and GTVs in the optimizer window and editing the dose levels and priorities however takes even longer than before.
From "Start VMAT Optimization", it took 6 minutes 10 seconds until the first iteration appeared.
(14 minutes into optimization with 25 lesions and 76 targets.)
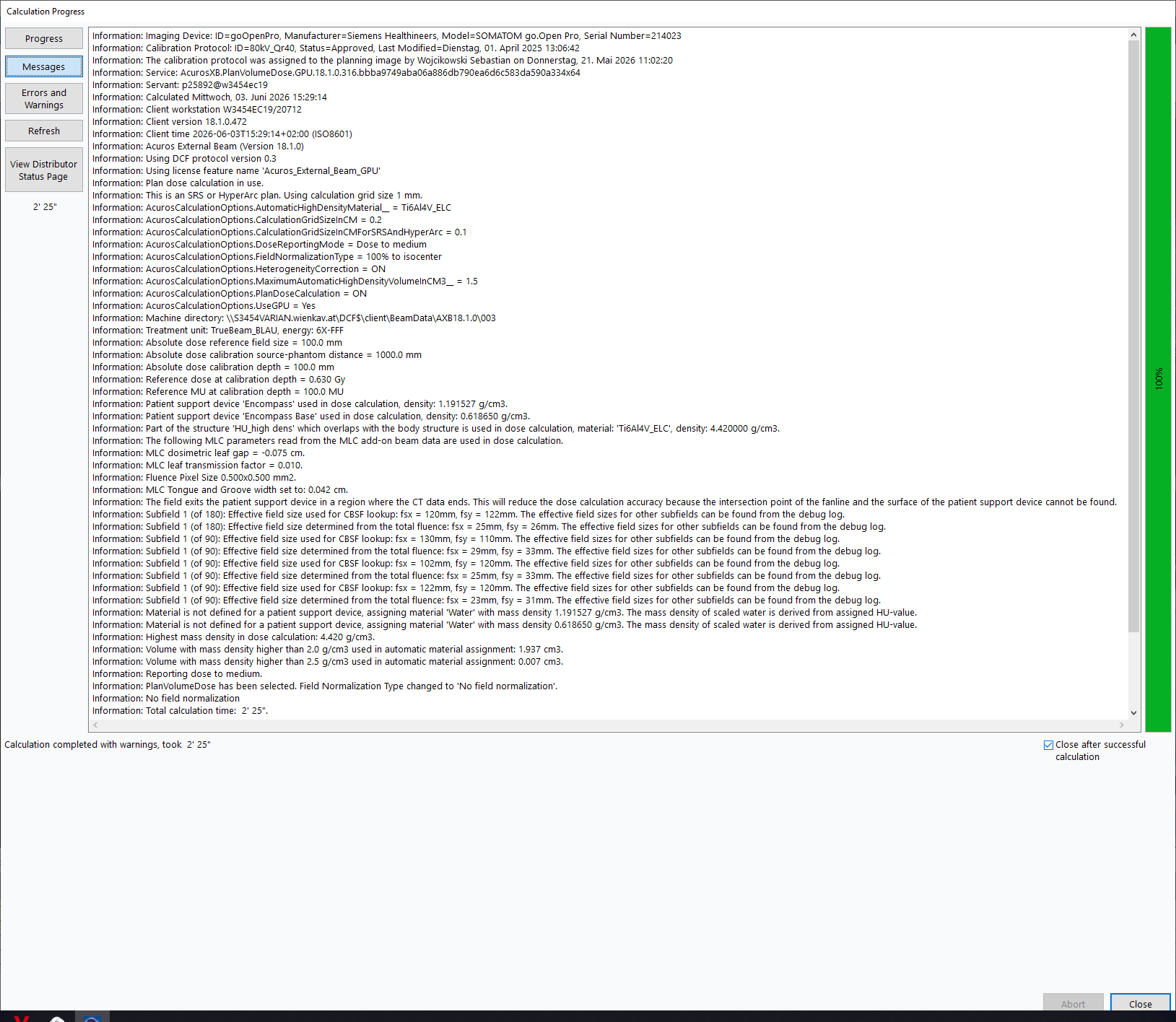
Intermediate Dose started after 35 min 40 sec. The final dose appeared after 62 minutes:
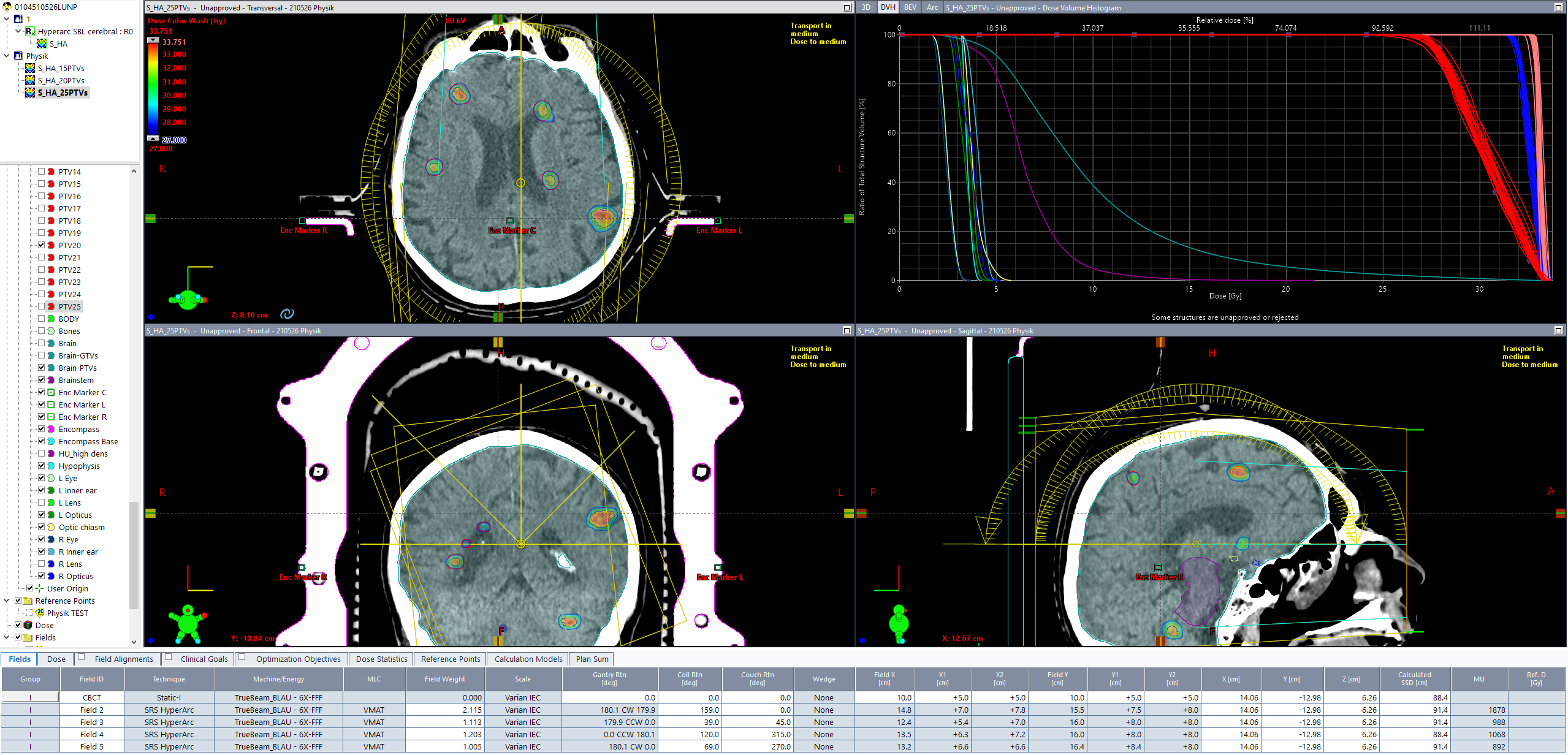
(Final dose for 25 lesions or 76 targets. Here is the calculation log.)
{kind=link}
The Final Challenge: 33 Lesions, 100 Targets
One bold step is necessary to test Eclipse's capability of handling 33 lesions or 100 targets. Adding eight more lesions means adding 8 x (GTV, CTV, PTV, ATV, BTV) = 40 new structures. This took 14 minutes 20 seconds in Contouring.
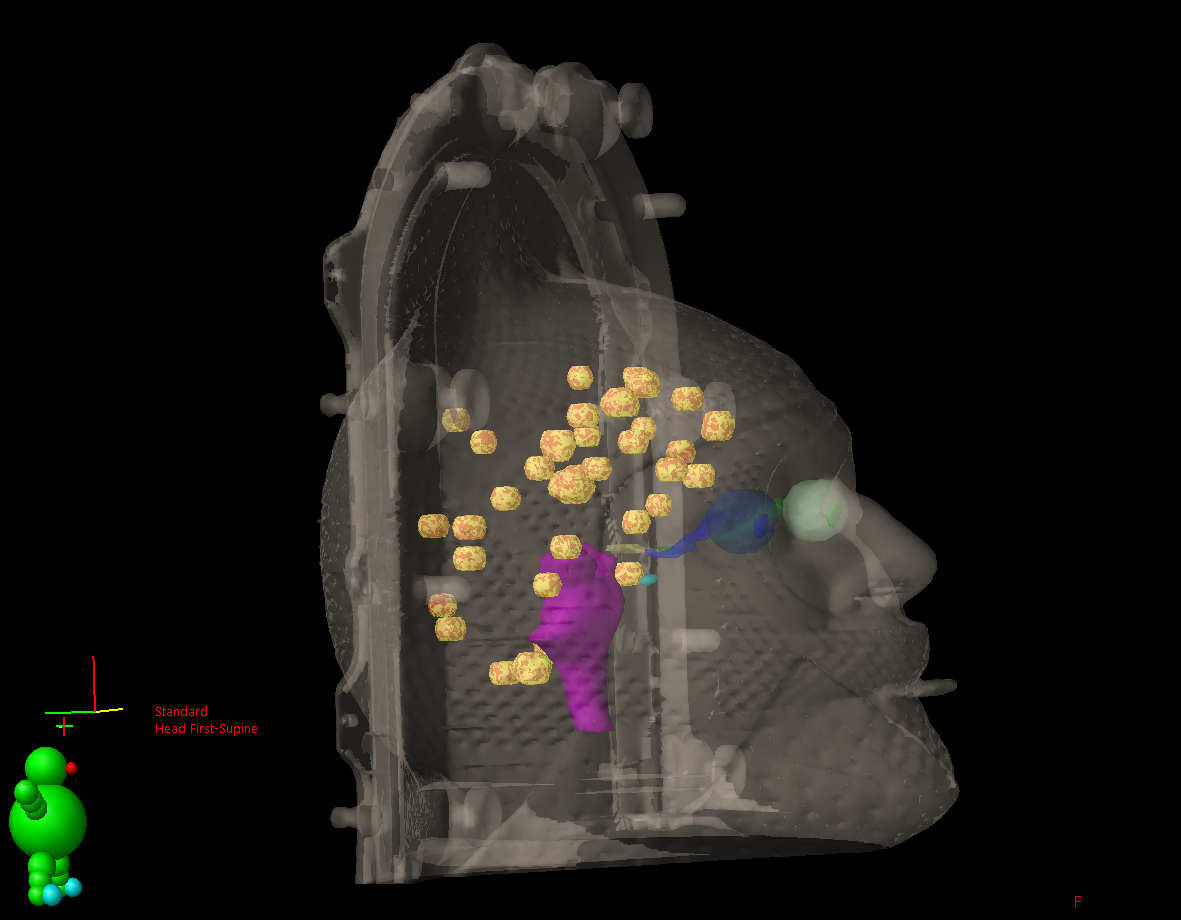
(Visualization of the 33 lesions.)
With "Modify HyperArc Plan", things start to get exciting.
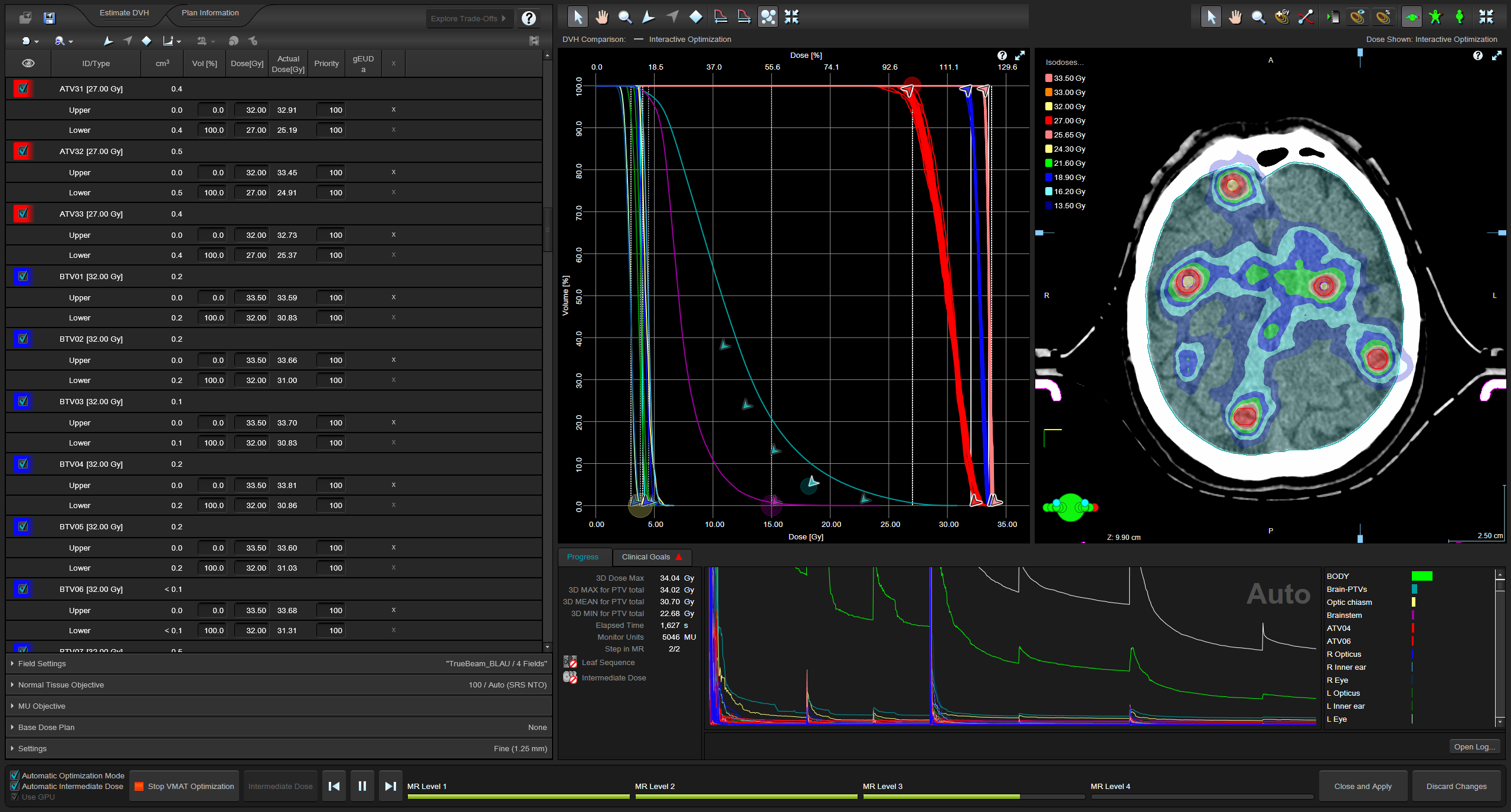
The target list is now 3 pages long. Exactly 100 targets are selected, if we also include the "PTV total" structure:
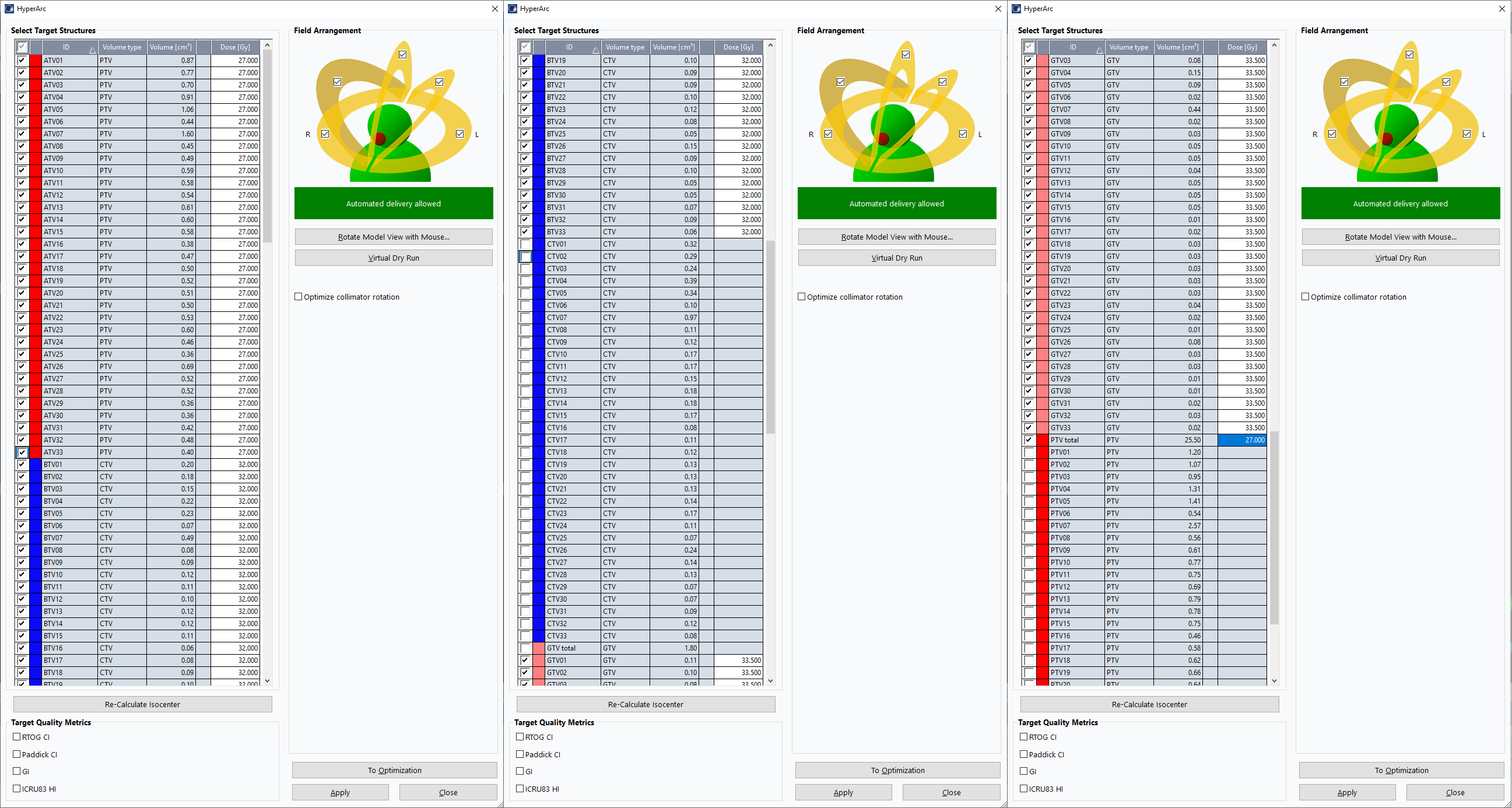
The response in the PO Optimizer window, as expected, is even slower than before. However, with some preparation and care, one can perform 10 to 15 clicks (such as "Ctrl+C" or "Ctrl+V") in advance by "clicking blind", without having to wait until the screen reacts. Preparation means that the area where all the clicks happen must be static on the screen, so that the edited field is still on the same screen location when the click is processed. No scrolling is allowed. This is why the following screenshot shows the structures GTV26 to GTV33:
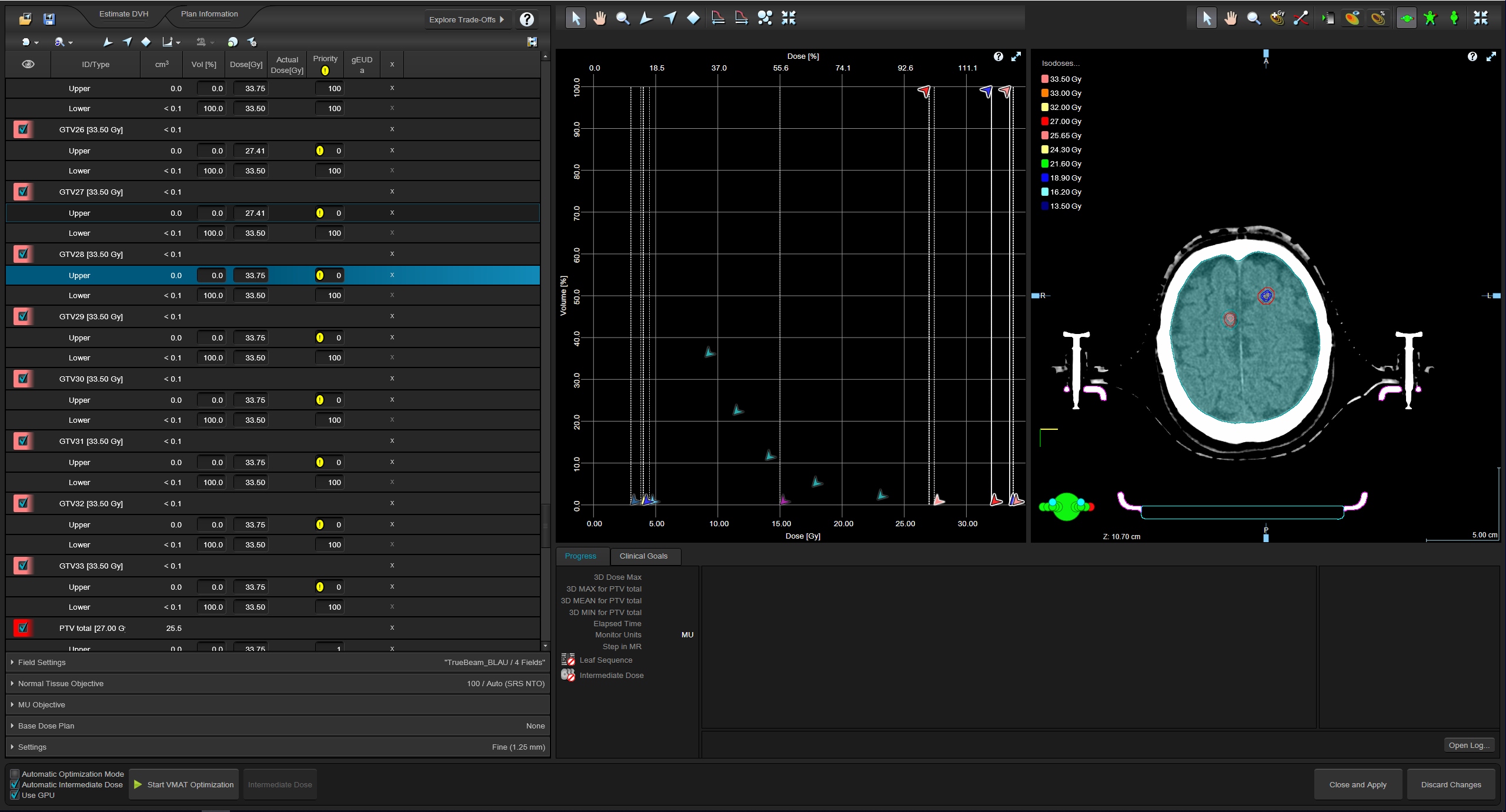
(Setting up an optimization of 100 targets. The list on the left has now a length of 13 pages!)
Doing the necessary edits (add "Upper", edit dose, edit Priority) for the 40 additional targets in the Optimizer window took 22 minutes.
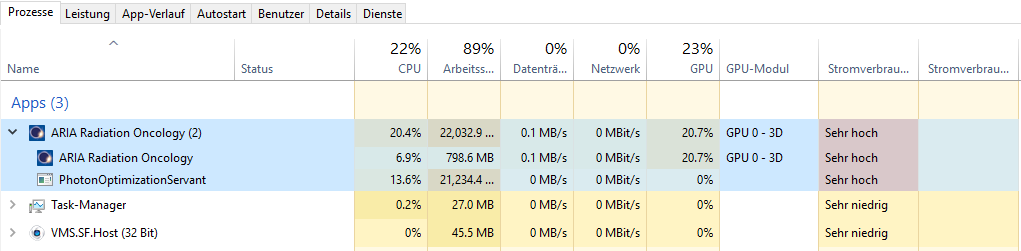
With 100 targets, it took 10 minutes until the first iteration appeared. RAM usage was about 89% during optimization.
Intermediate dose started after about 43 minutes. The complete optimization cycle for 100 targets including dose calculation (MR Level 1 - 4, Intermediate Dose, MR Level 3 - 4, Final Dose) took 71 minutes.
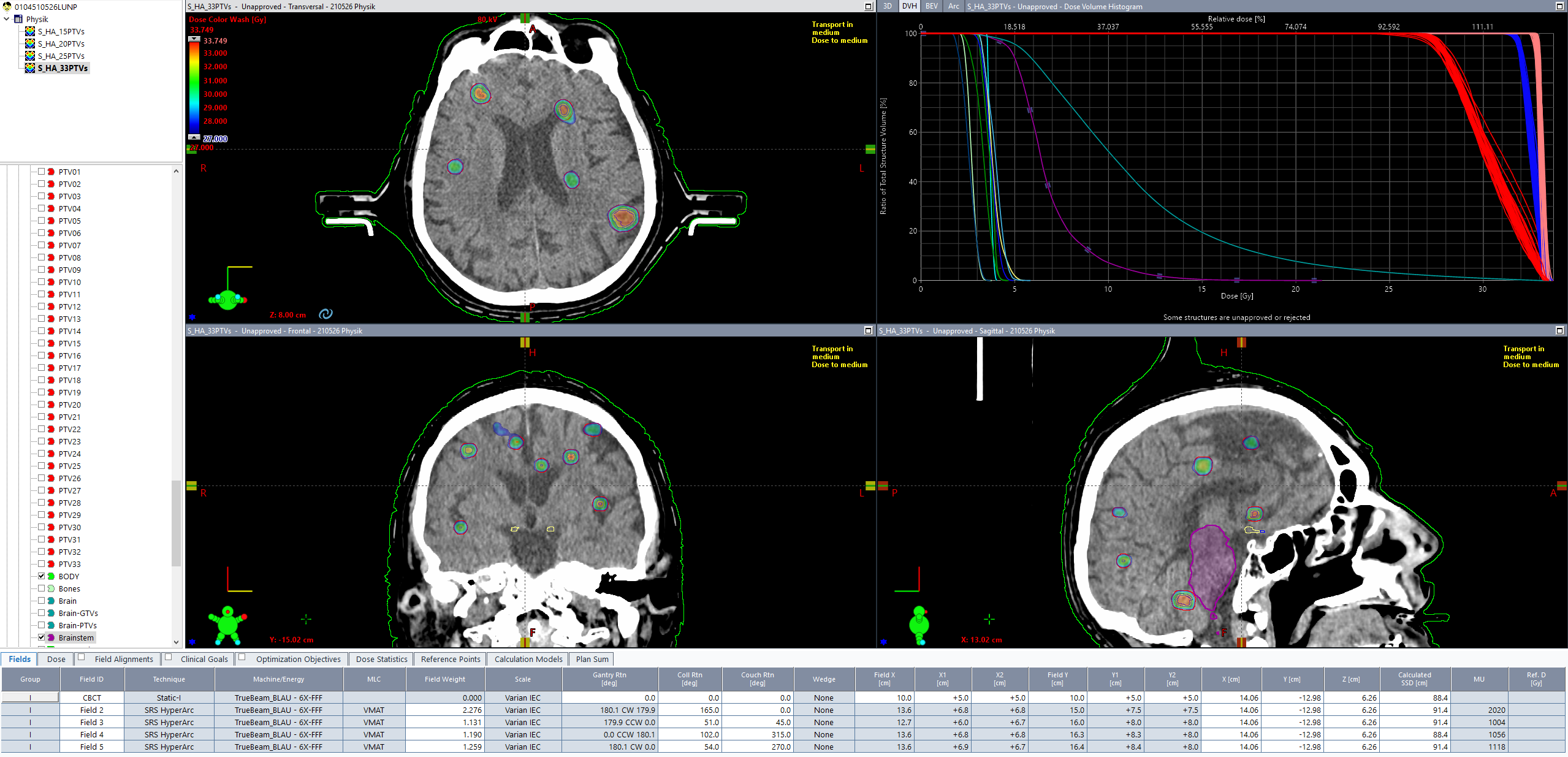
(Final dose distribution for 33 lesions, 100 targets.)
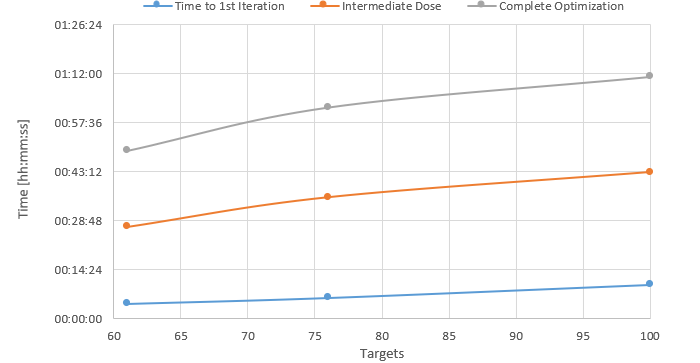
The timing for the three target sets (61, 76, 100 targets), as mentioned in the text, is plotted here:
Dosimetric Verification
One thing still needs to be checked: can such a plan be dosimetrically verified in the usual way with VERIQA? What if VERIQA cannot handle 100 targets?
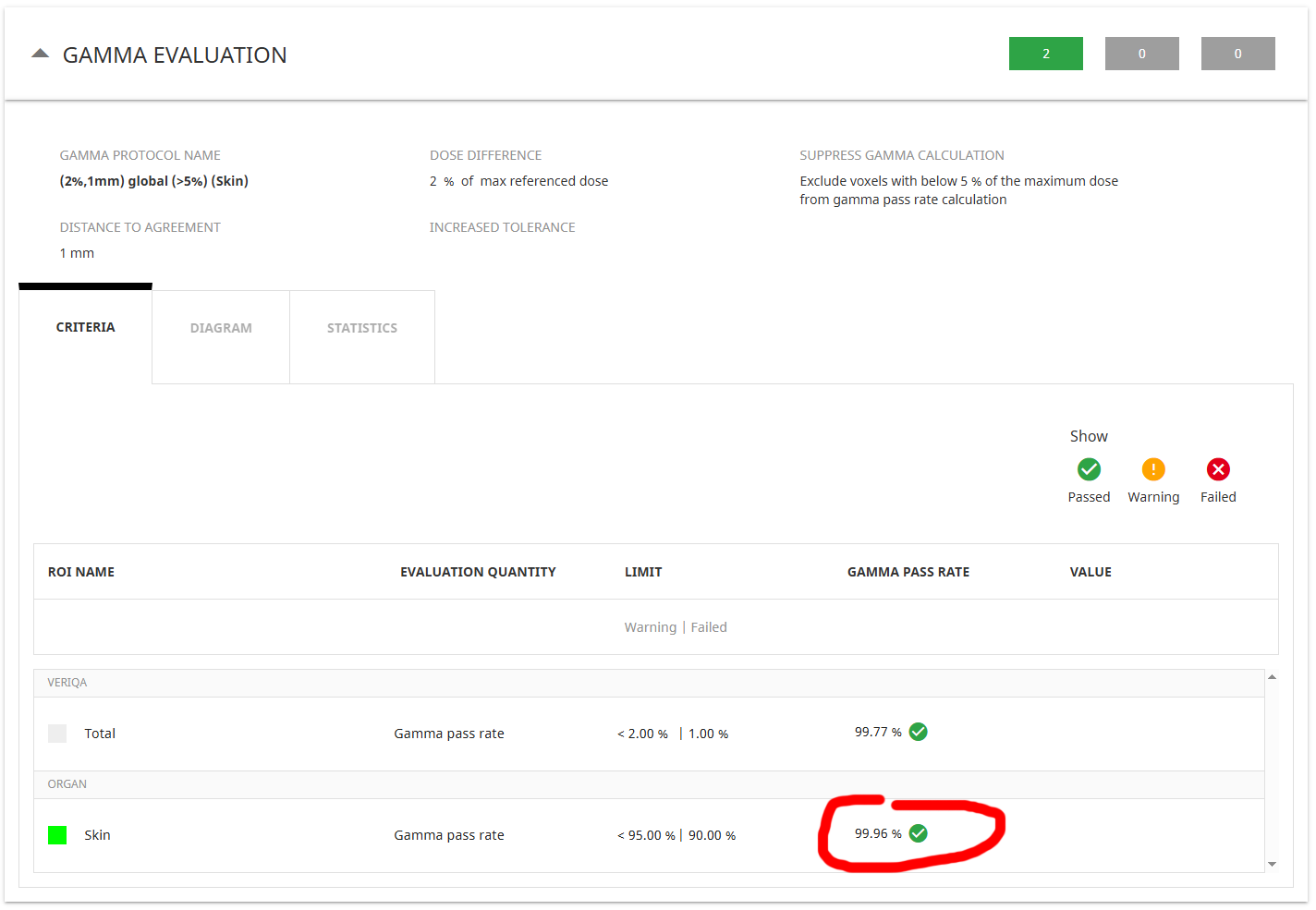
We sent the plan to VERIQA (current version: 3.0.36) as it is, and applied a 2%/1mm Gamma (GAM21) test to the Skin structure (5% cutoff).
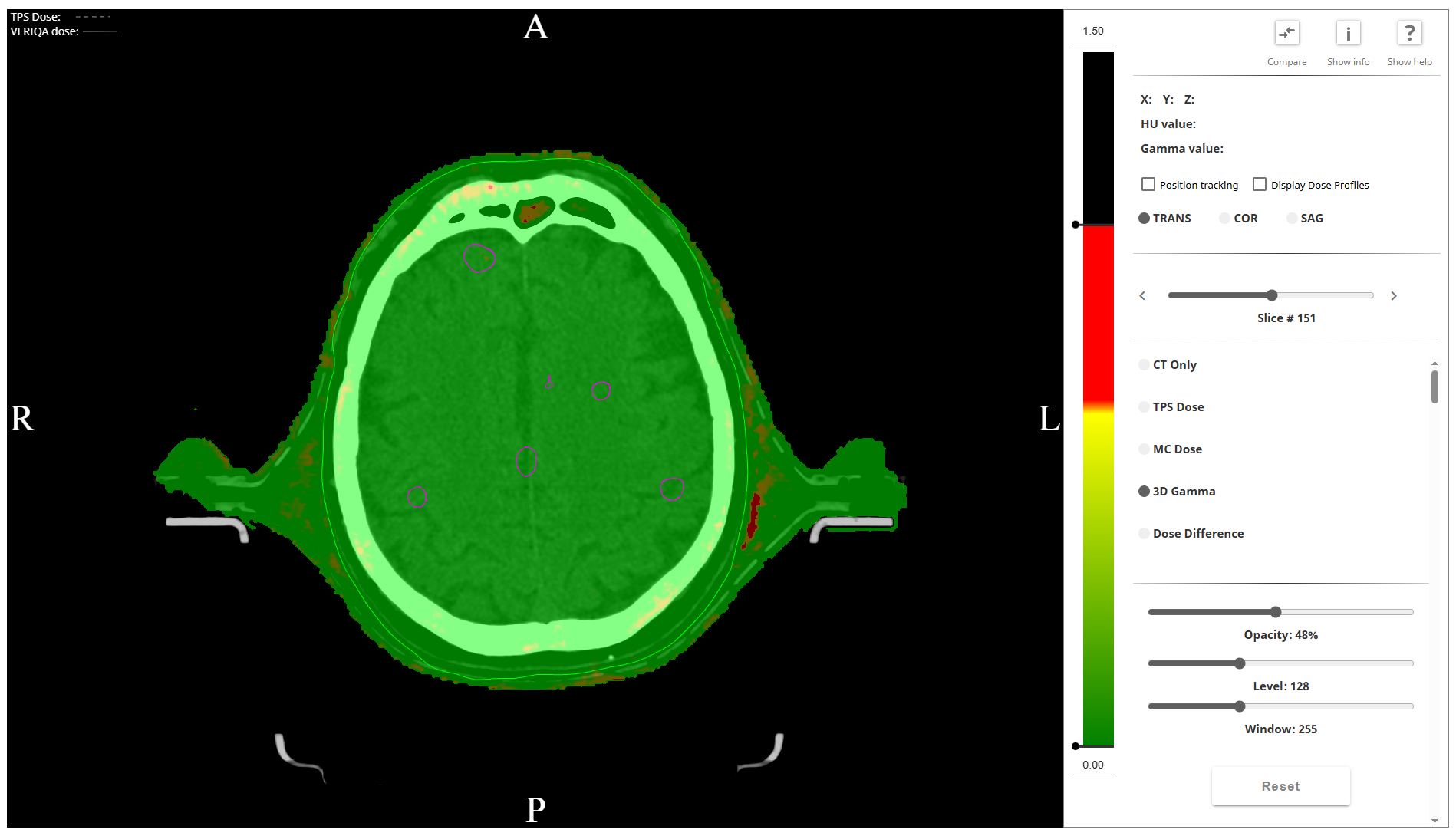
(The Skin structure is visible as a light green line around the skull - where it is expected to be.)
The GAM21 passing rate for the Skin structure was 99.96%:
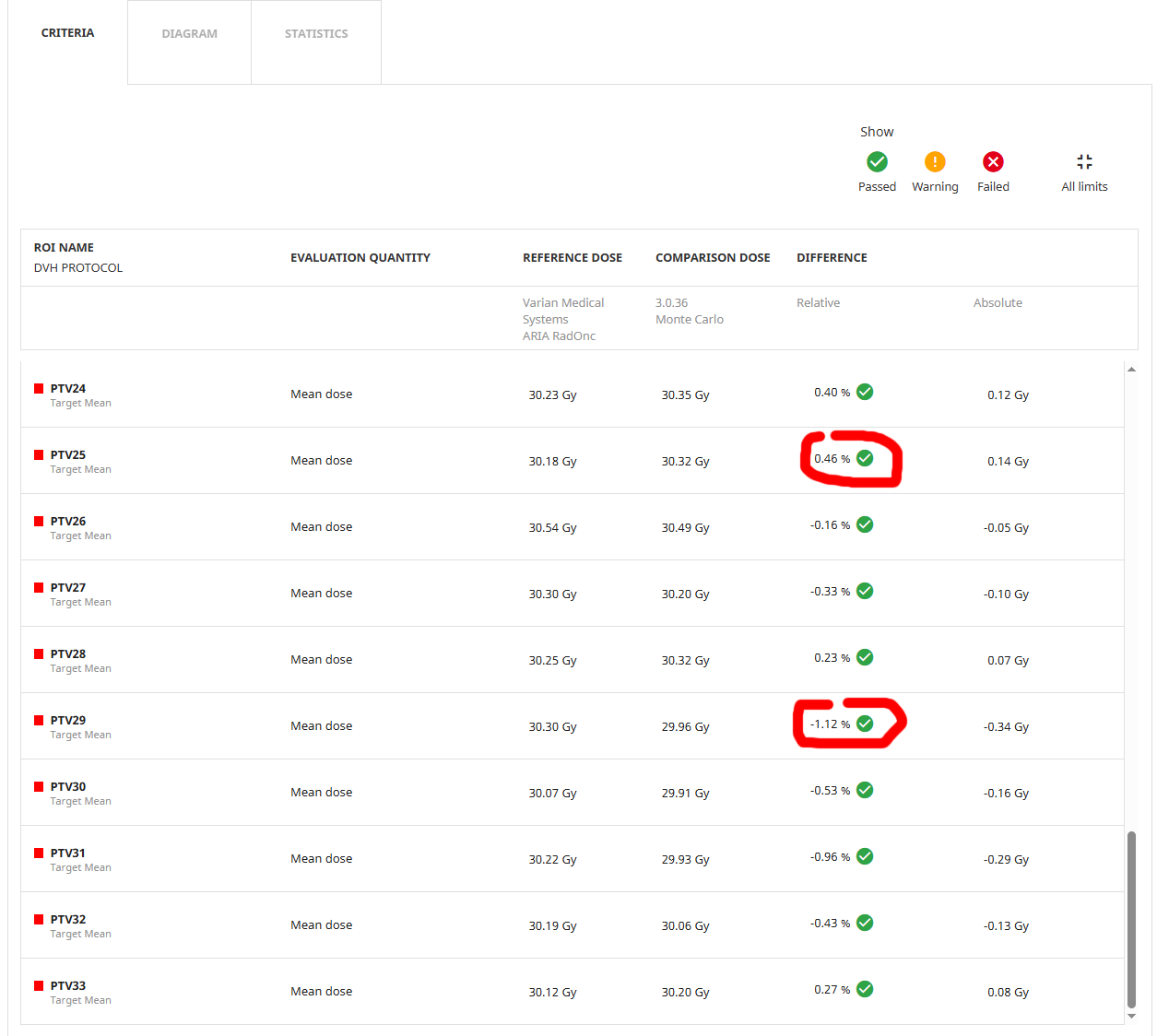
The relative mean dose deltas in percent for the 33 individual PTVs ranged from -1.12% to +0.46% (luckily, the extremes are on the same page):
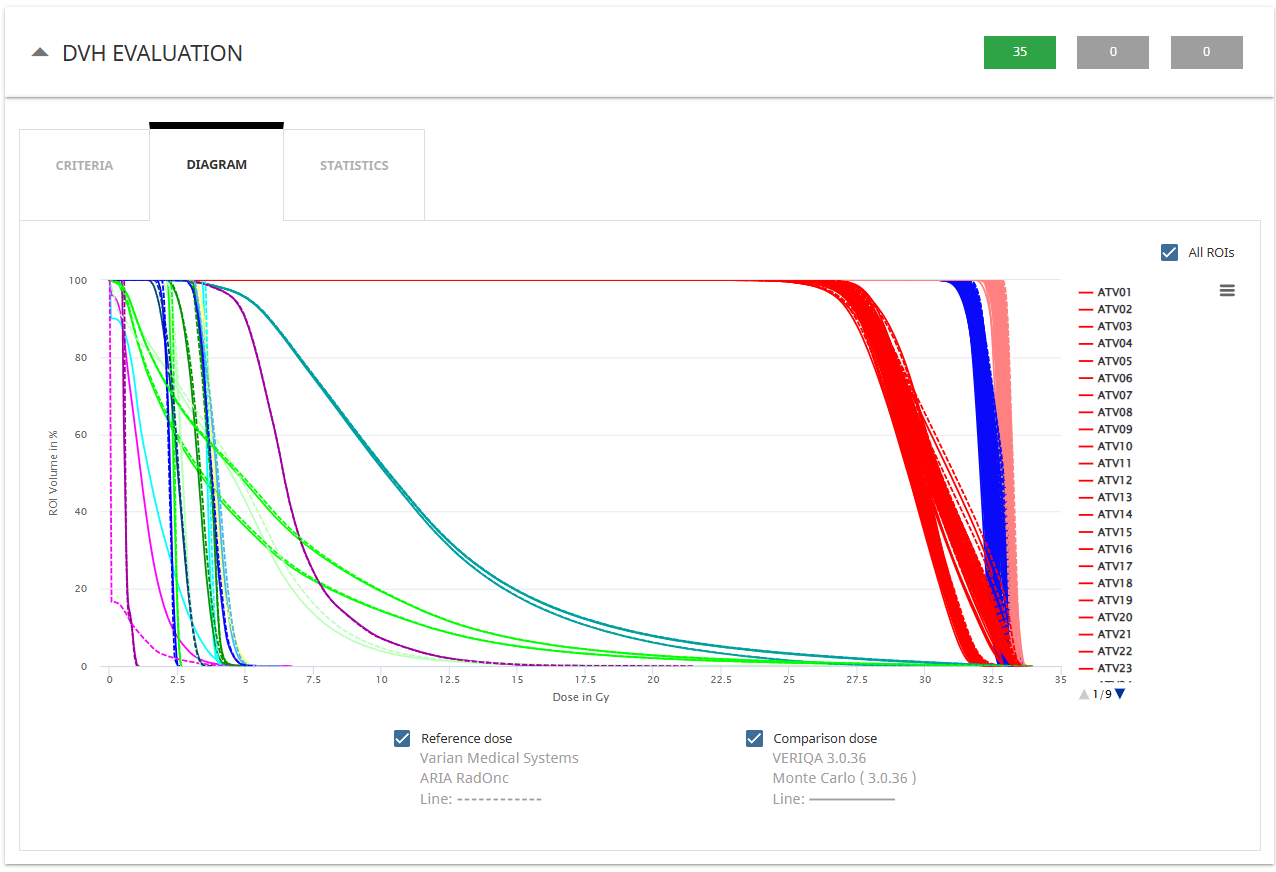
The individual DVH curves can be compared, but the "All ROIs" diagram lacks some clarity (better select the ROIs one after another):
The conclusion is: VERIQA has no problem with such plans.
Discussion
We have demonstrated that HyperArc plans with 33 lesions and 100 targets can be optimized, calculated, and verified. We'll leave it at that: 100 is a nice round number.
By incrementally adding more targets, no absolute limit could be determined. The system simply seems to slow down during editing5. For a plan with 100 targets, the time for optimization and dose calculation was a moderate 71 minutes.
From a clinical perspective, the question naturally arises: Does it make sense to irradiate 33 lesions? However, it's certainly good to know that it's possible, just in case ...
Notes
1Different lesions can be optimized to receive different doses in a HyperArc plan, but for simplicity, we choose the same prescribed dose for each lesion.
2As described, we sometimes add more structures as Targets, such as PTV total. This is optional. From previous optimizations, we got the impression that convergence is faster if PTV total is added to the target list, even if the Priority of its dose objectives is set to only 1.
3Only one goal according to the Timmerman tables for three fraction was missed in the clinical plan, which says that the V23Gy of the Brain-GTVs structure should be < 5 cm3. This is practically not achievable for multi-met plans and our margin settings. The situation worsens when more lesions are added.
4Remember that the sole purpose of this study is to find out whether the TPS is able to handle a large number of structures (targets).
5Memory consumption is about 26 GB during the last optimization with 25 lesions.