VERIQA Acceptance and Commissioning
After the successful "launch of the rocket" and some fine-tuning, we structured the acceptance tests into the following categories:
- Validation of absolute dose
- Open fields
- Static MLC fields
- Small fields
- Simple IMRT fields
- Complex IMRT fields
- Testing of the Couch model
- Clinical plans (on CT data of patient anatomy)
All tests in the list, except the last item, are performed in water. Most of the plans are calculated on a 30x30x30 cm cube, some on a cylindrical phantom of 30 cm diameter. The clinical plans cover the full spectrum of complexities, AAA and AXB, and also involve some density overrides and material assignments1.
All together, 86 plans were evaluated for acceptance.
For each acceptance evaluation in VERIQA, we calculated the global Gamma (2%/2mm) Agreement Index (GAI22) of the BODY structure, calculated with a dose cutoff of 10% and a precision of at least 1%.
For each category, we report the worst and the best GAI22 result.
Results
Absolute Dose
Actually it is not necessary to check absolute dose separately, because VERIQA evaluations are always absolute. However, since DCC was not modified beyond the PTW recommentations expressed in their Configuration Protocol, we were excited about the results. Plans were 10x10 cm fields in calibration geometry (SSD 100 cm), all energies, AAA and AXB. No dose bias was observed.
- 99.46% < GAI22 (absolute dose) < 100%
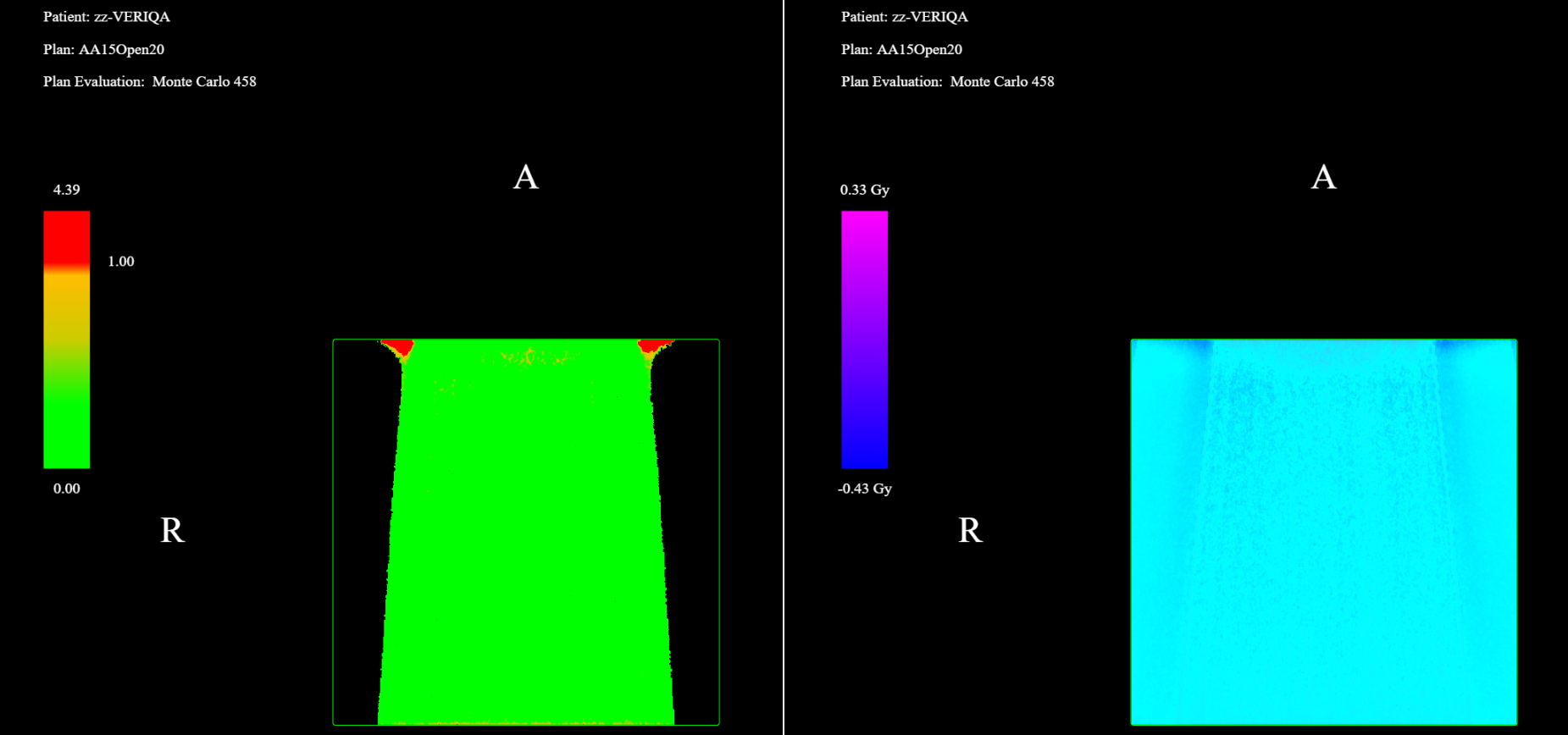
Open Fields
The open fields (AAA) were selected according to the PTW recommendation for acceptance testing (VERIQA - Customer Beam Model Acceptance Protocol): 4x4 cm, 10x10 cm, 20x20 cm.
- 98.0% < GAI22 (open fields) < 100%
The largest deviation (GAI22 = 98%) was observed for the 15X, 20x20 cm field, in the region of electron contamination close to the surface. Left is Gamma, right is dose difference:
Static MLC Fields
PTW recommends to check abutting static MLC fields, in order to verify MLC calibration (LOC). We created several variants. In one of them, the abutment edges of the five fields in the plan were not straight but designed like a jigsaw puzzle. This also reveals the tongue and groove effect:
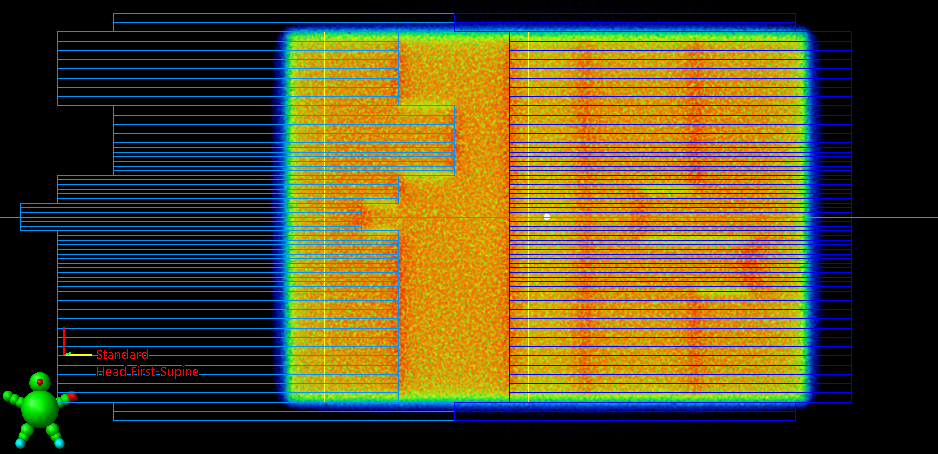
AAA, AXB and MC reproduce this effect correctly in the profiles:
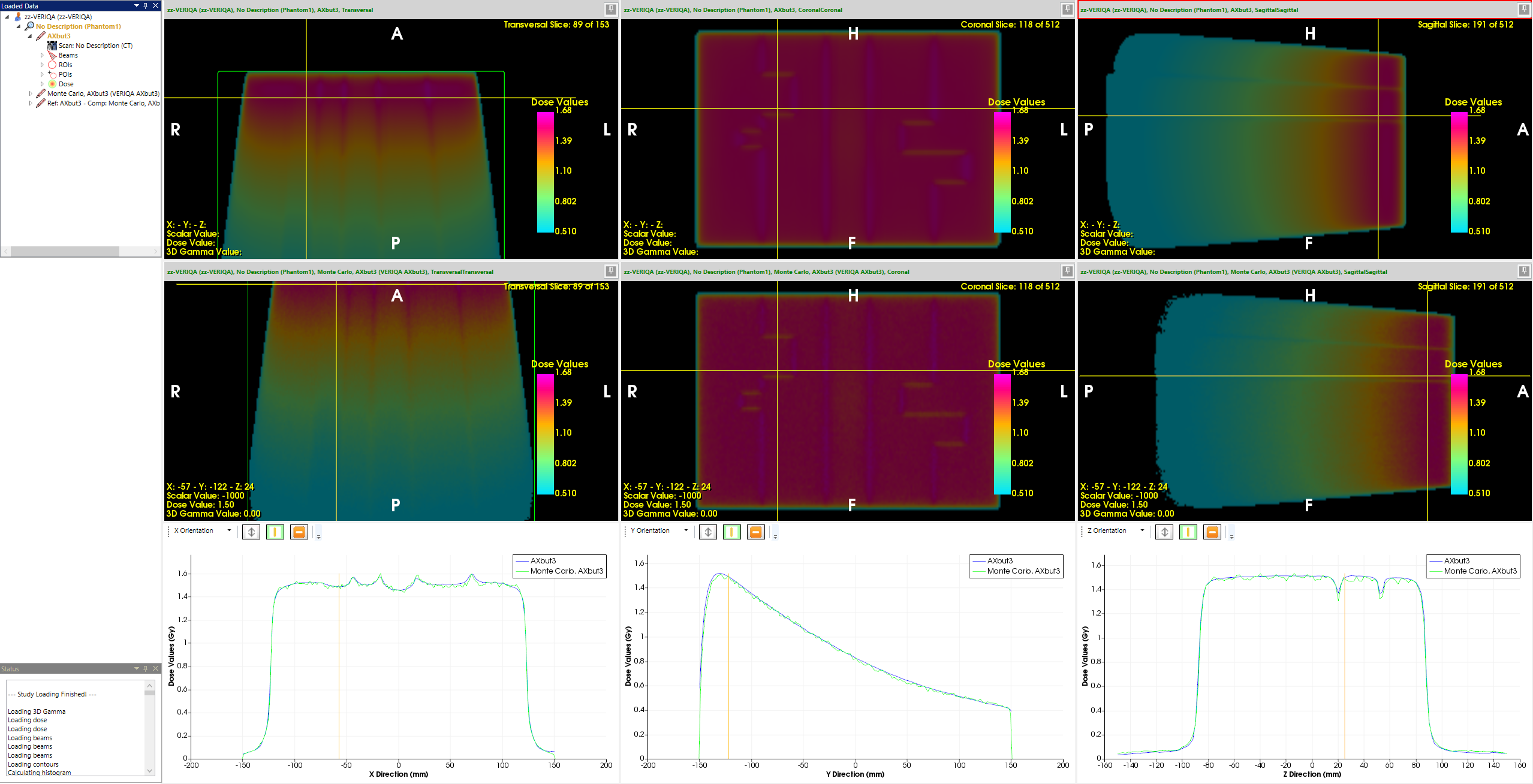
- 99.66% < GAI22 (static MLC fields) < 99.76%
Small Fields
We calculated 1x1 cm (jaw-defined) static fields without MLC, plus a 0.5x0.5 cm (MLC) field with the jaws set to 3x3 cm. In the latter, two leaf pairs of the HD120 MLC are open by 0.5 cm, since the leaf width at isocenter is 0.25 cm.
We calculated the fields on a cylindrical phantom (diameter: 30 cm) for the 6FFF energy, AAA and AXB.
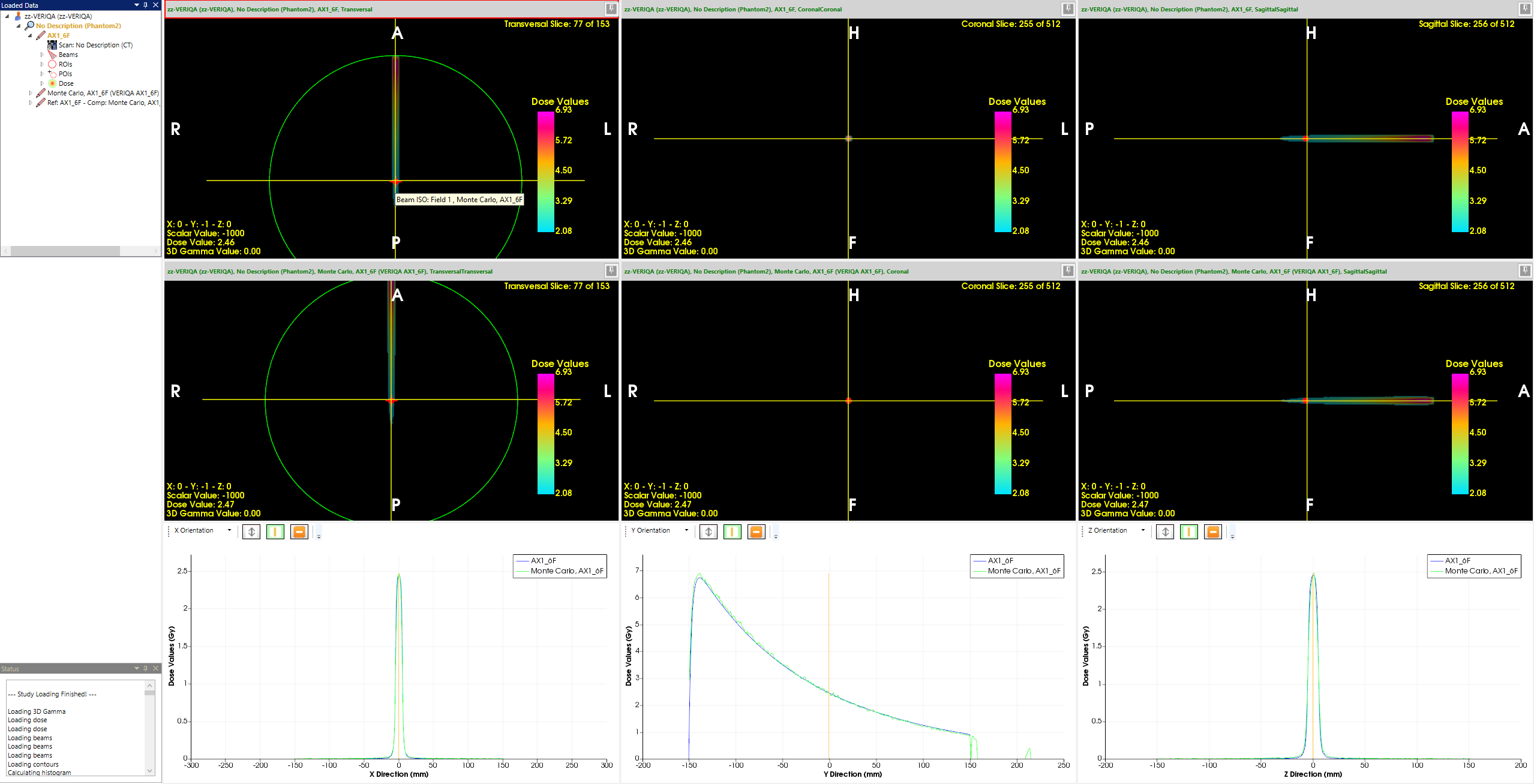
(The 1x1 cm jaw field. Profile shape and absolute dose show excellent agreement. GAI22 = 100%)
The even smaller 0.5x0.5 cm MLC-defined field with a jaw setting of 3x3 cm is hard to visualize in RT View, because the field has the same width on the screen as the yellow crosshairs. Zooming in helps a little:
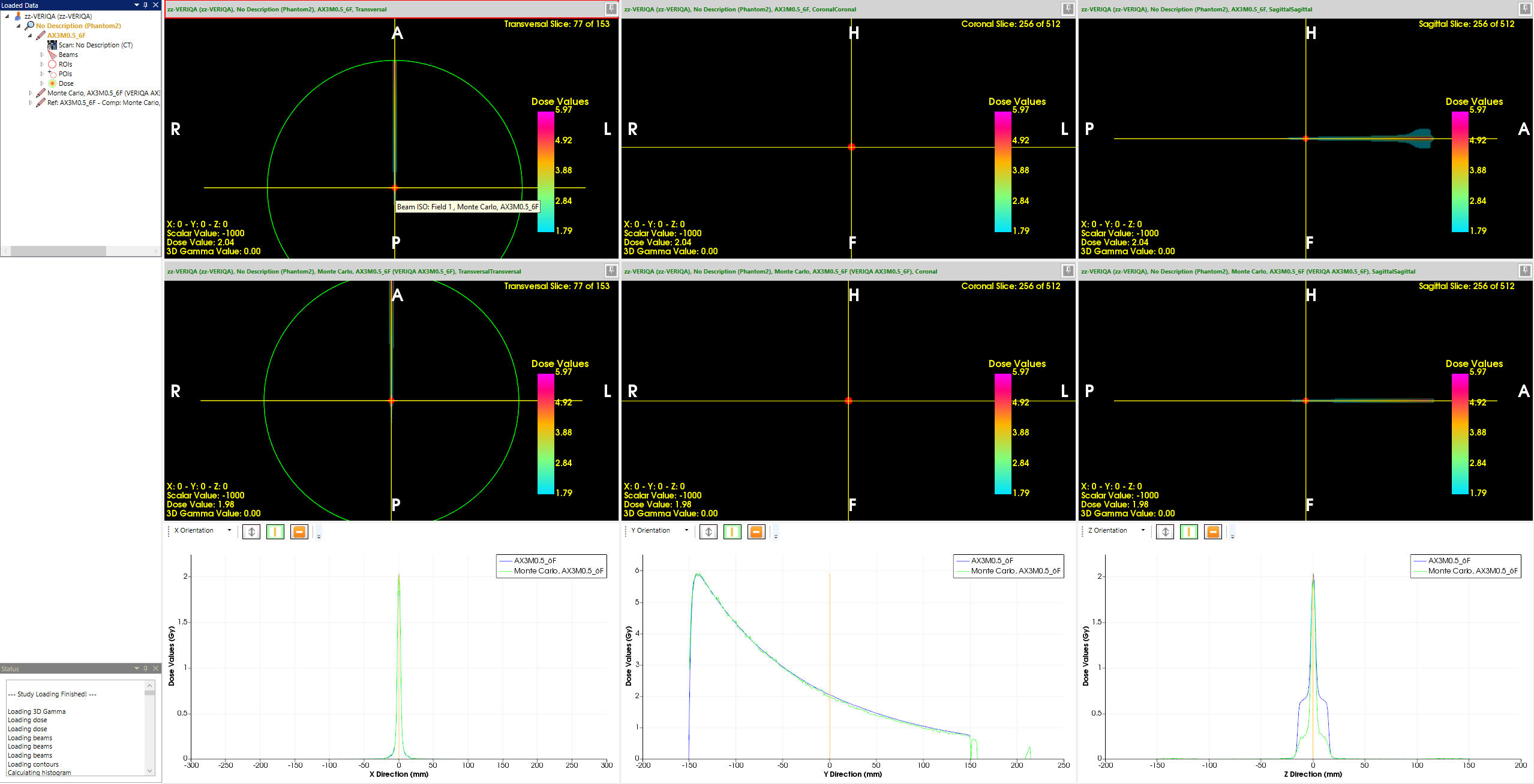
(The 0.5x0.5 cm MLC field. Shape of transverse profile and depth dose are still excellent.)
The agreement for small fields is remarkable.
- 95.42% < GAI22 (small fields) < 100%
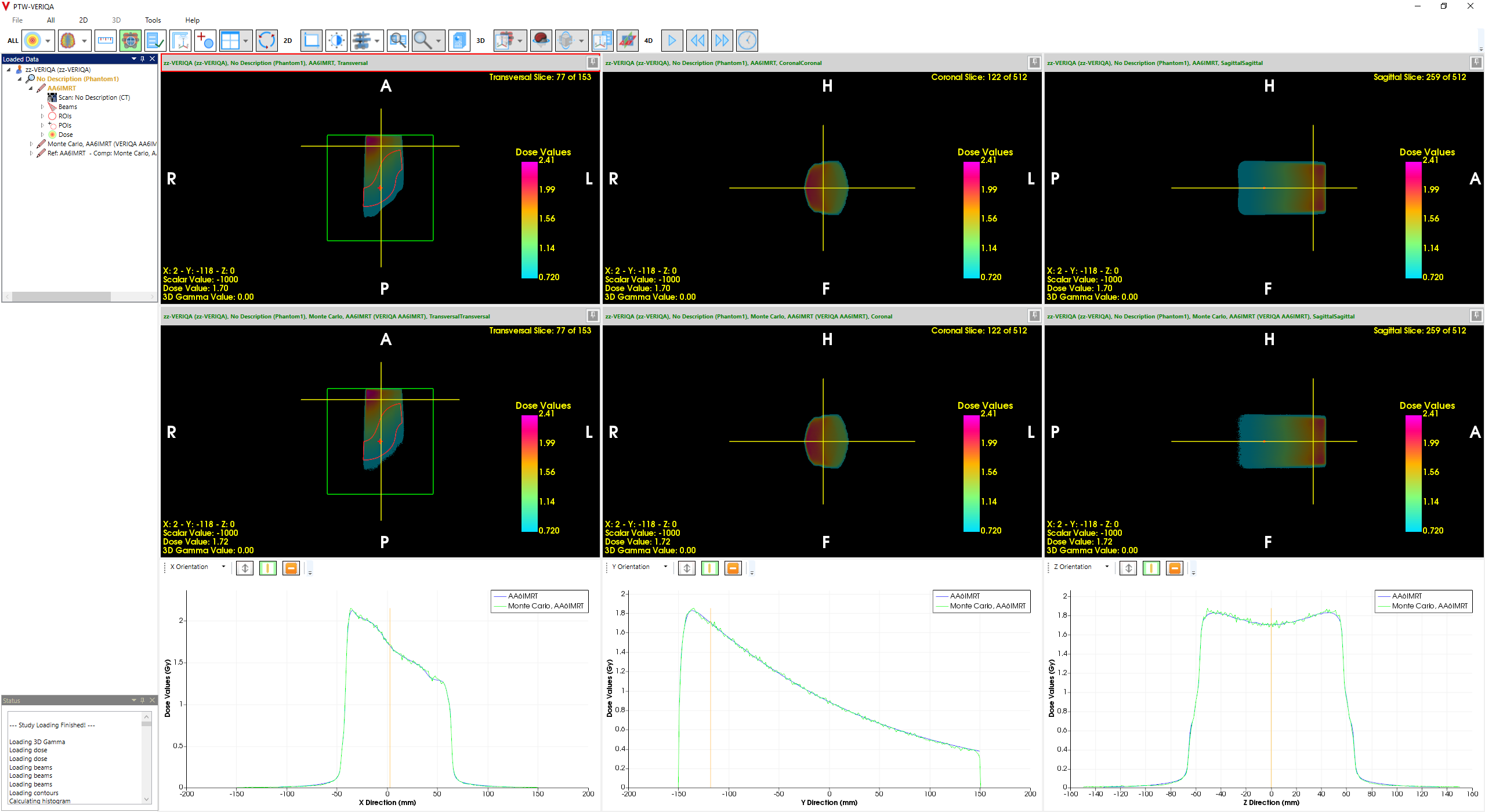
Simple IMRT Fields
Following the PTW recommentation for acceptance setups, we created simple IMRT fields of low complexity on an artificial target.
{kind=link}
- 99.38% < GAI22 (simple IMRT fields) < 100%
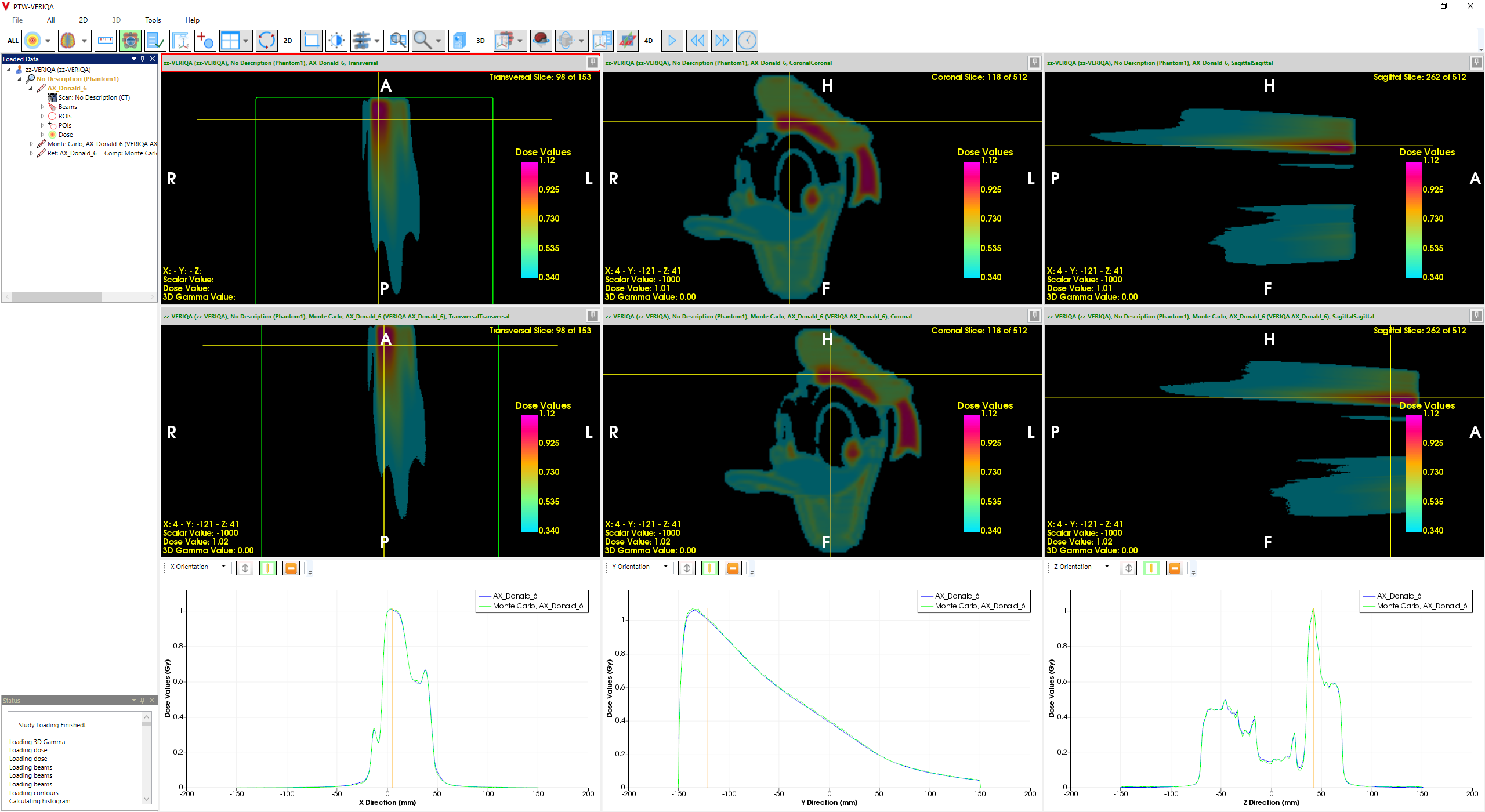
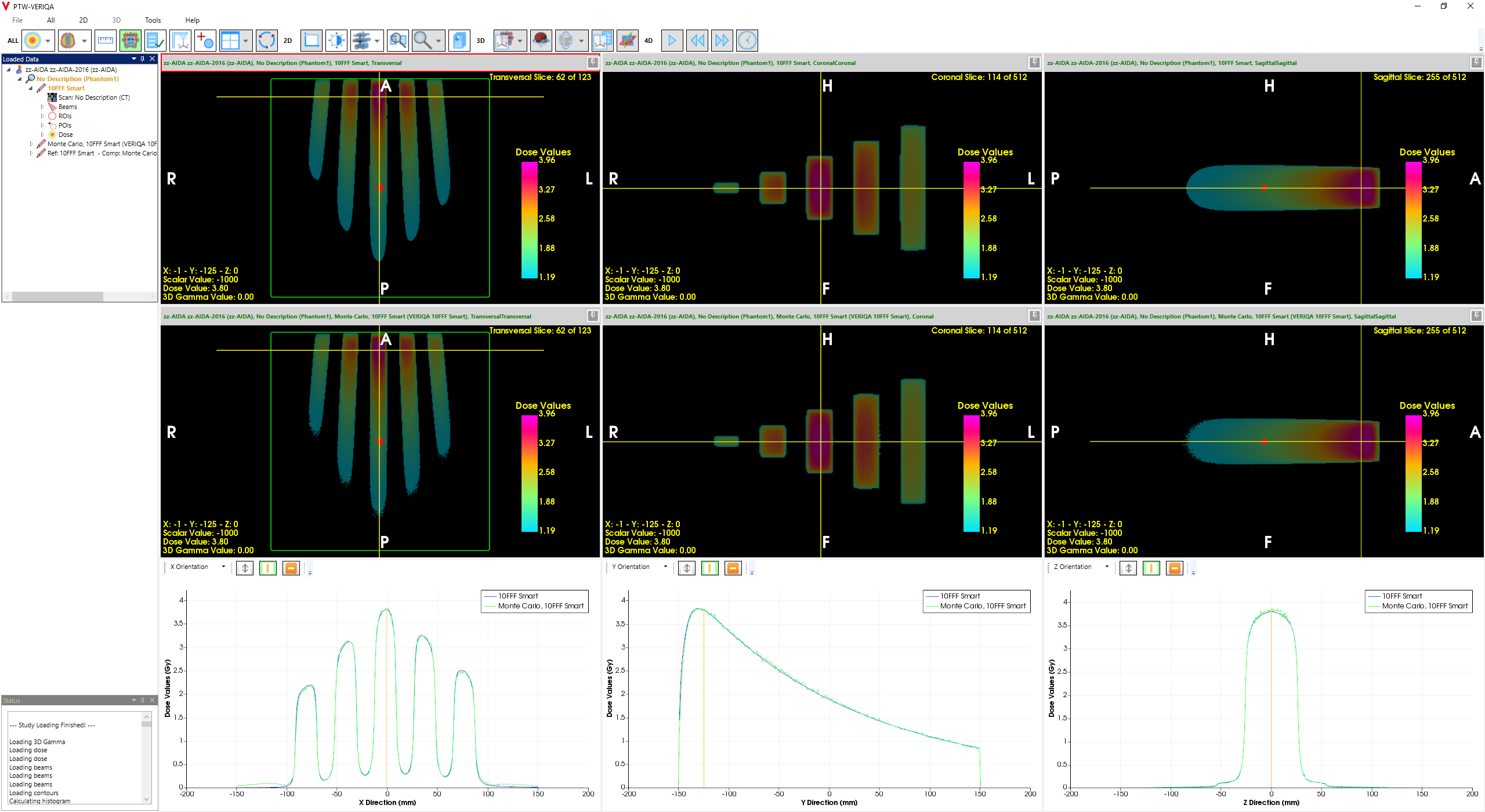
Complex IMRT Fields
The well-known "Donald" pattern is a typical example, but also the "Chair" (see below) and "AIDA" patterns are on the list.
{kind=link}
{kind=link}
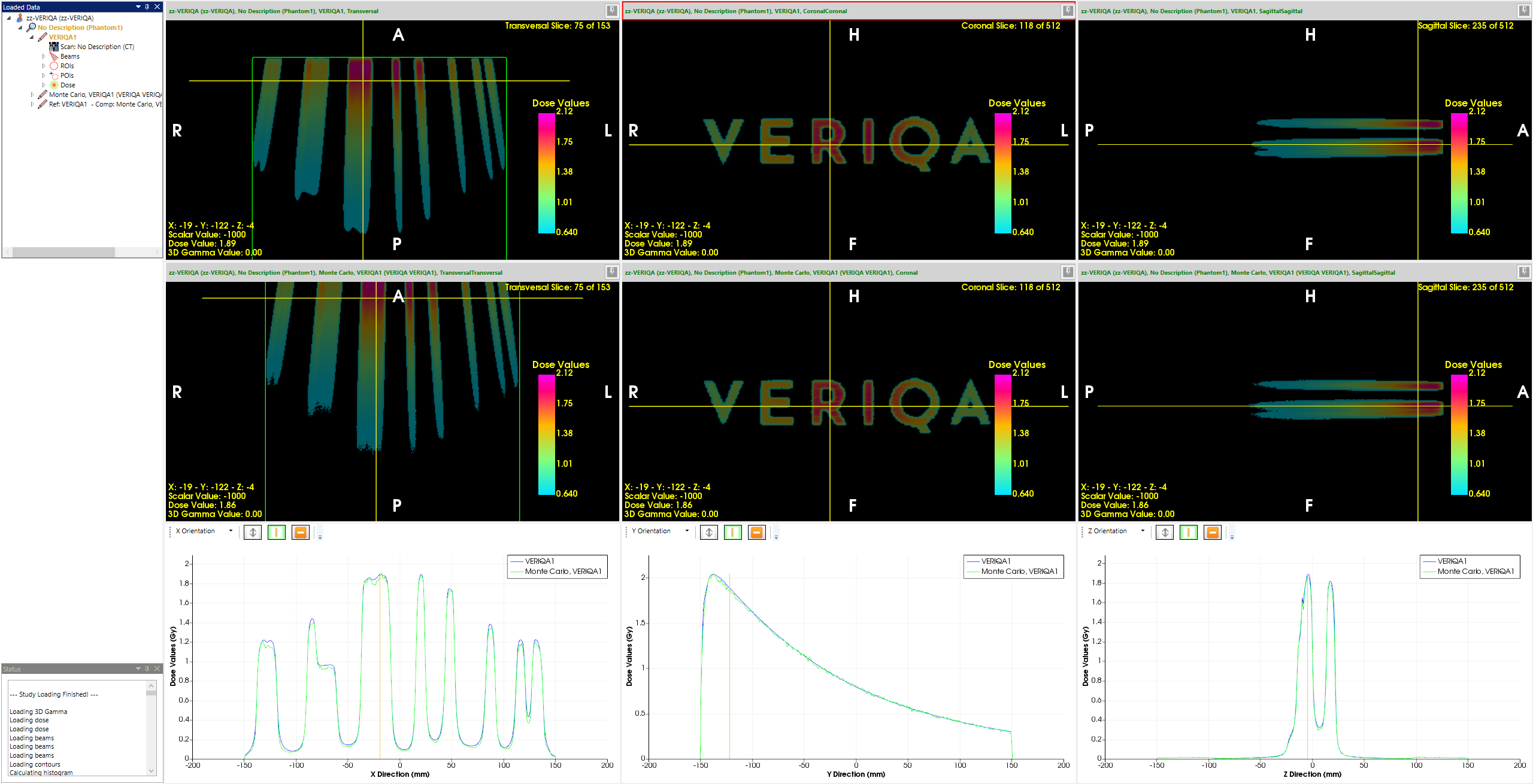
A new example is the VERIQA logo, here calculated with AAA. The 6FFF field has 2000MU@1400MU/min and 3 carriage groups. Jaw tracking is ON.
The GAI22 of this highly complex field is 99.66%. The profiles also match very well:
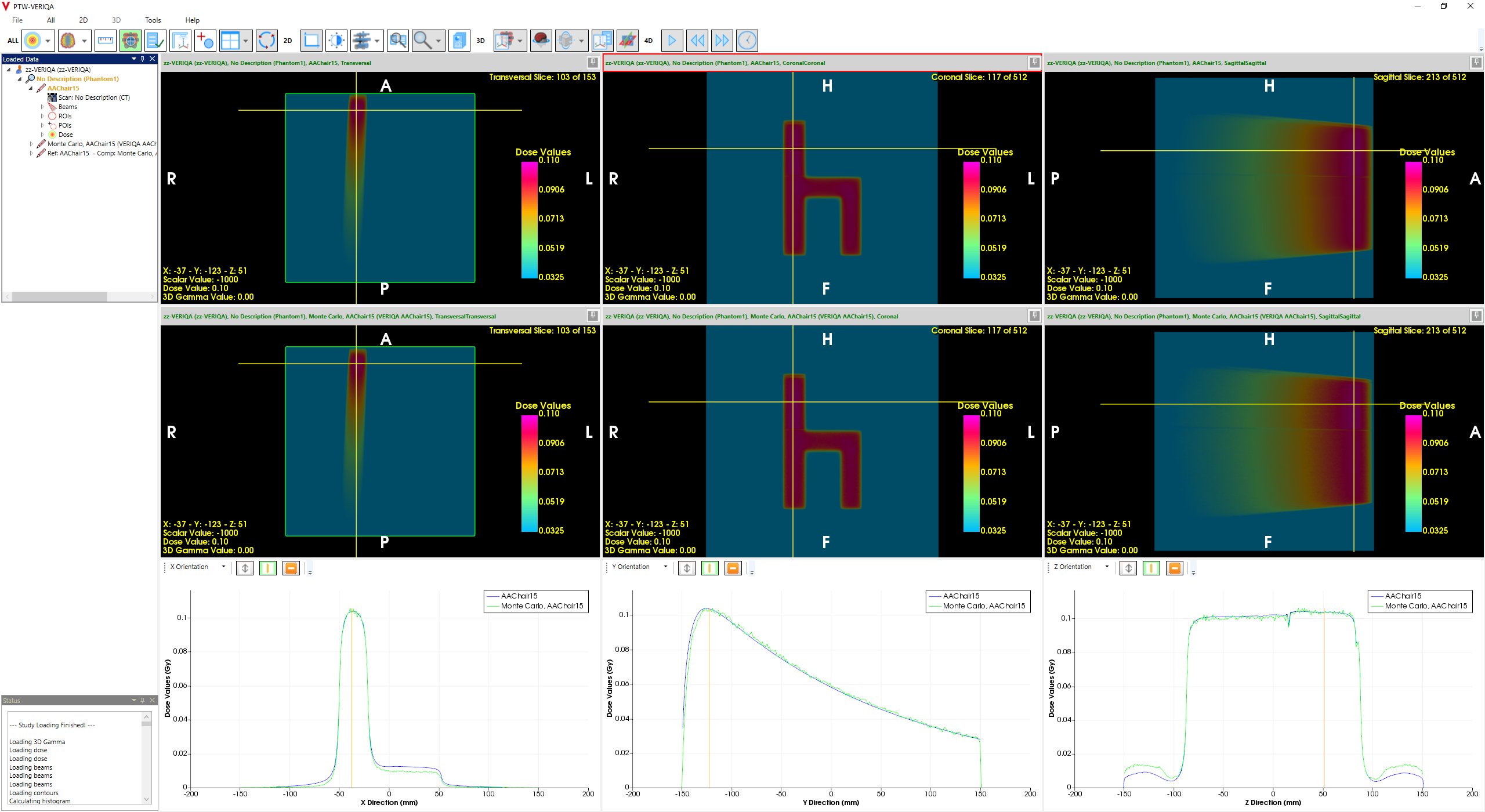
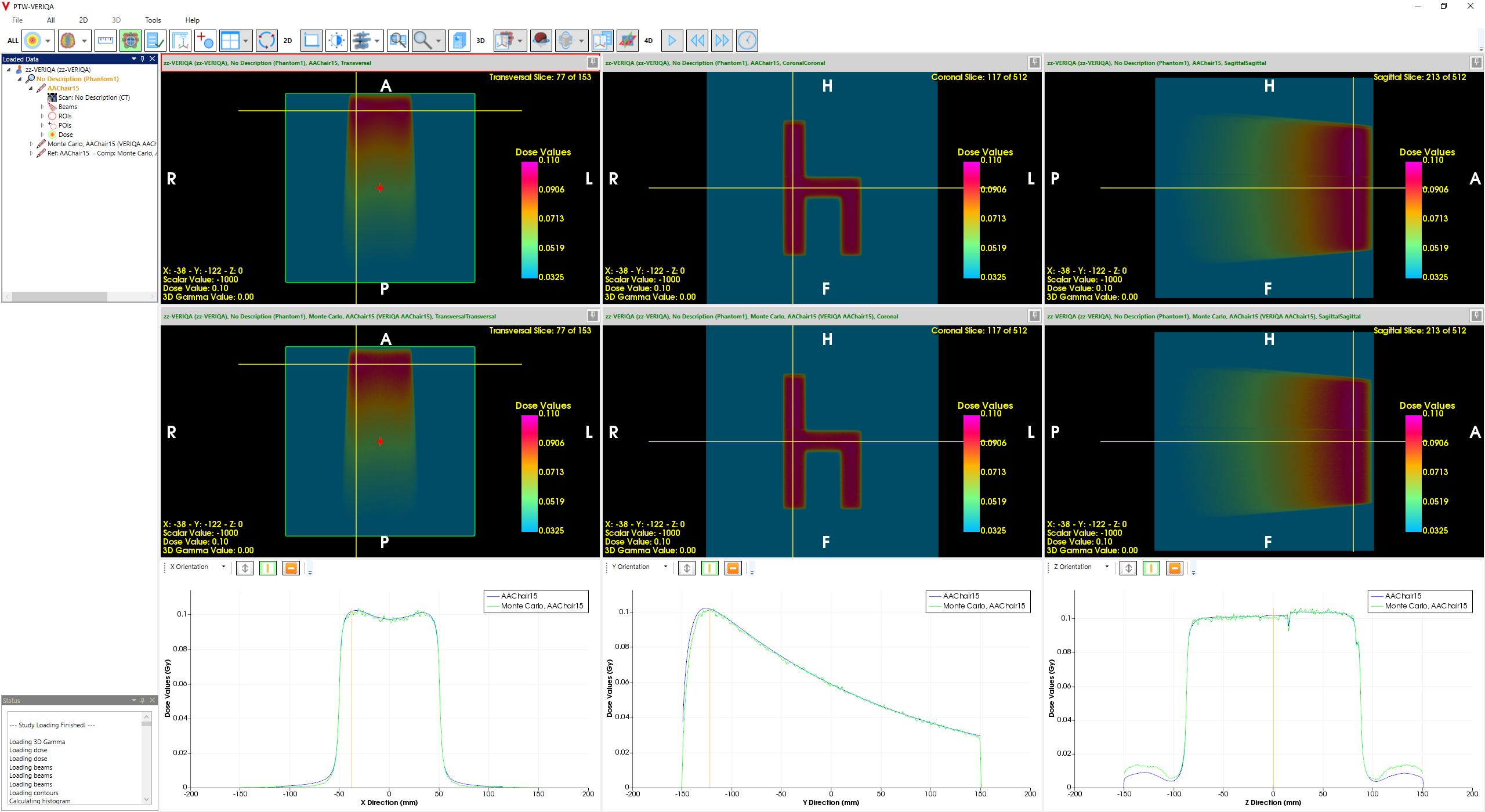
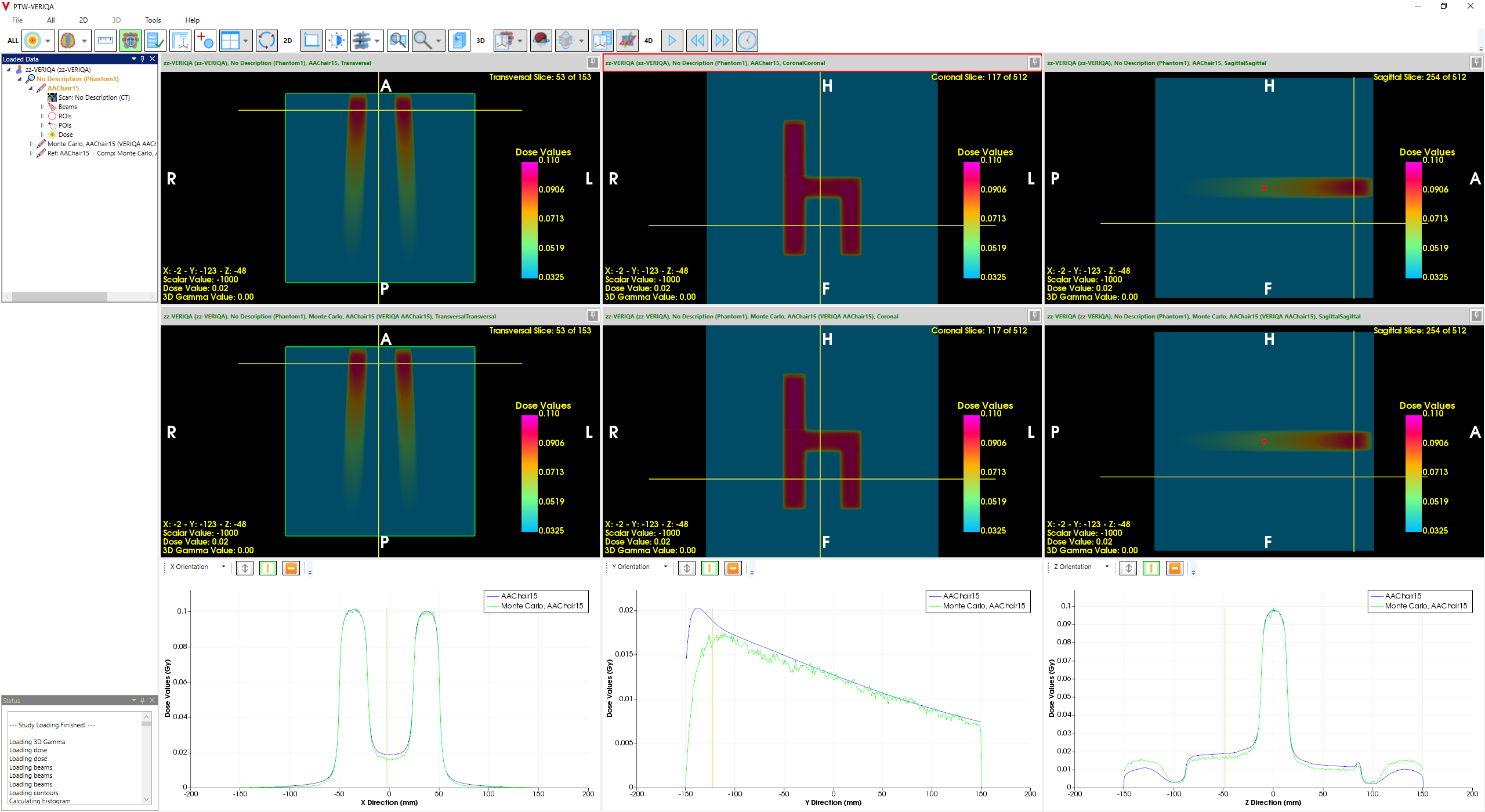
The lowest GAI22 (92.32%) is for the rather demanding "Chair" test pattern, 15X, calculated with AAA. Here, the doseage of the Chair is rather low (prescription dose 0.2 Gy, 59 MU), which forced the Leaf Motion Calculator (Smart LMC) to generate a moving gap with only 3.5 mm width in the back of the Chair (upper part of the pattern):
(The Chair demonstrates static transmission in the upper right quadrant, gap transmission between the legs.)
See the profiles across the back, the seat and the legs of the Chair: Static leaf transmission seems to be a little too low in the MC model, if we assume the TPS profile is correct2.
{kind=link}
{kind=link}
{kind=link}
- 92.32% < GAI22 (complex IMRT fields) < 100%
Testing of the Couch Model
These tests mainly consist of oblique fields that partly penetrate the couch from below:
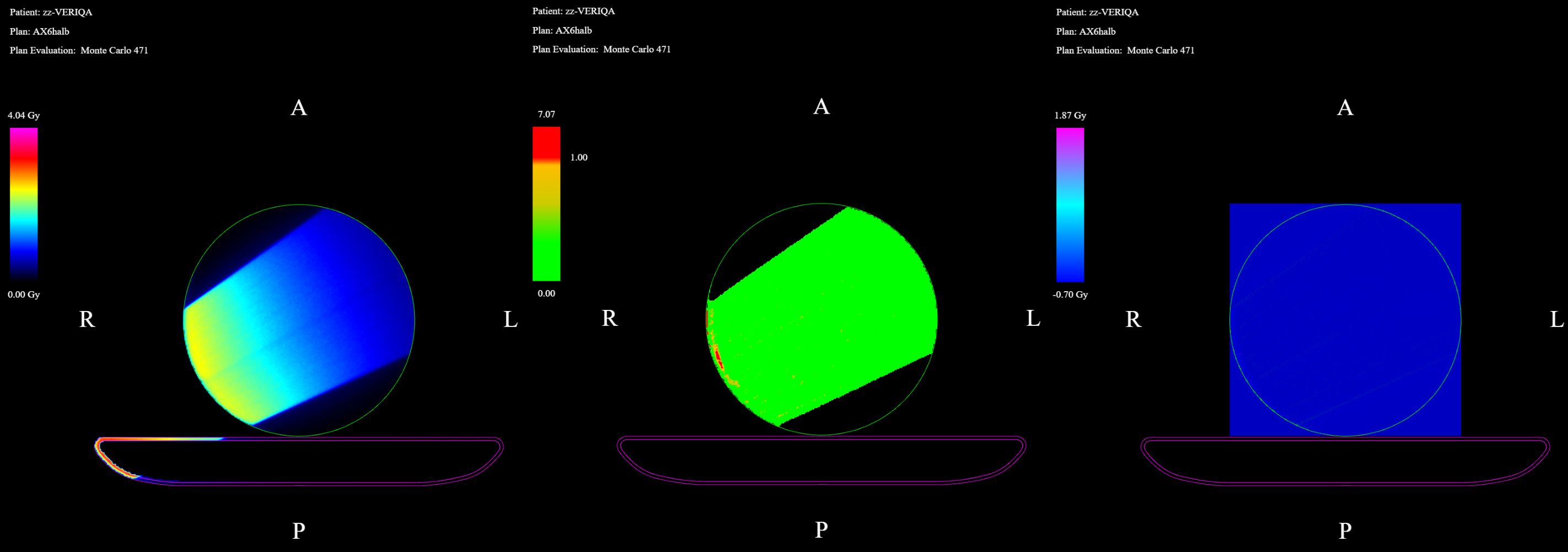
(Partial couch penetration, 6X, AXB. Left: MC, Middle: GAM22, Right: dose difference.)
In clinical situations, this can happen during breast treatments, if the lateral fields have a steep angle. Agreement is typically better for AXB than for AAA, because AXB better handles the second buildup after couch penetration.
- 98.68% < GAI22 (couch model) < 99.98%
Clinical Plans
Some examples of clinical plans evaluated for VERIQA acceptance:
- Hybrid IMRT breast plan with Simultaneously Integrated VMAT Boost (SIB),
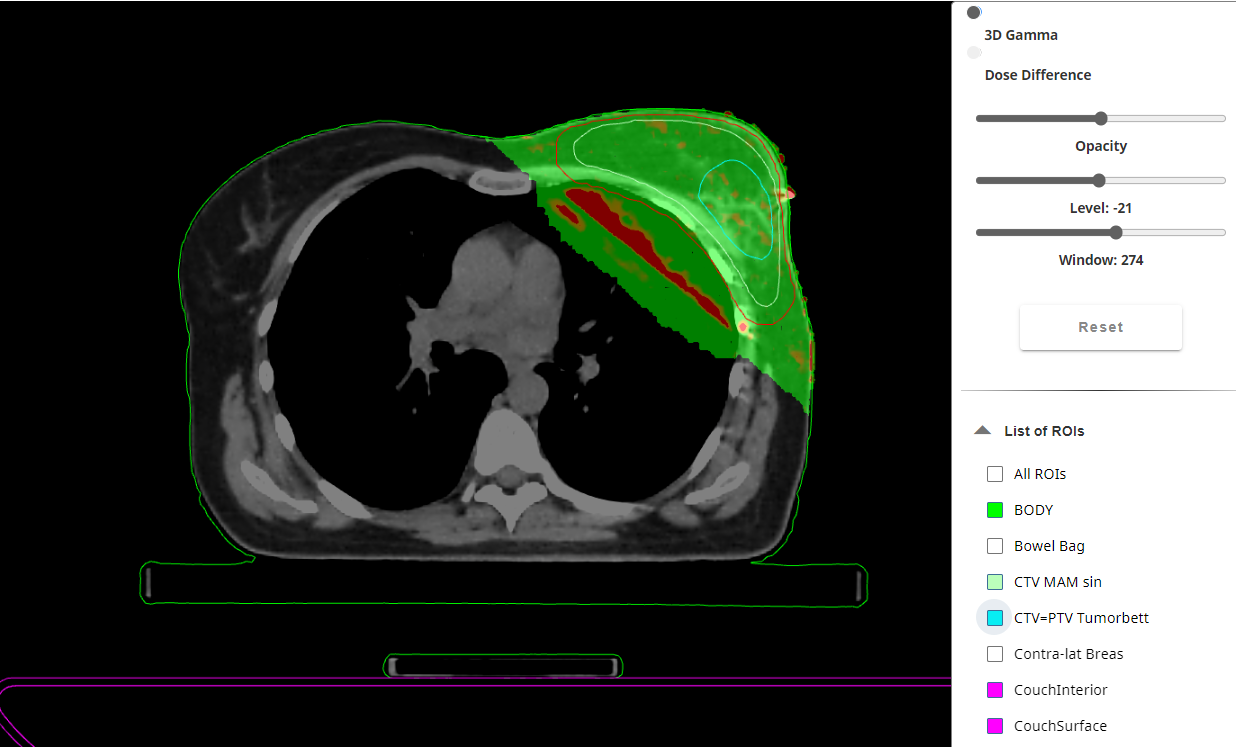
(Hybrid breast IMRT with SIB (one VMAT Arc), 6X, AAA. GAI22 = 95.52%)
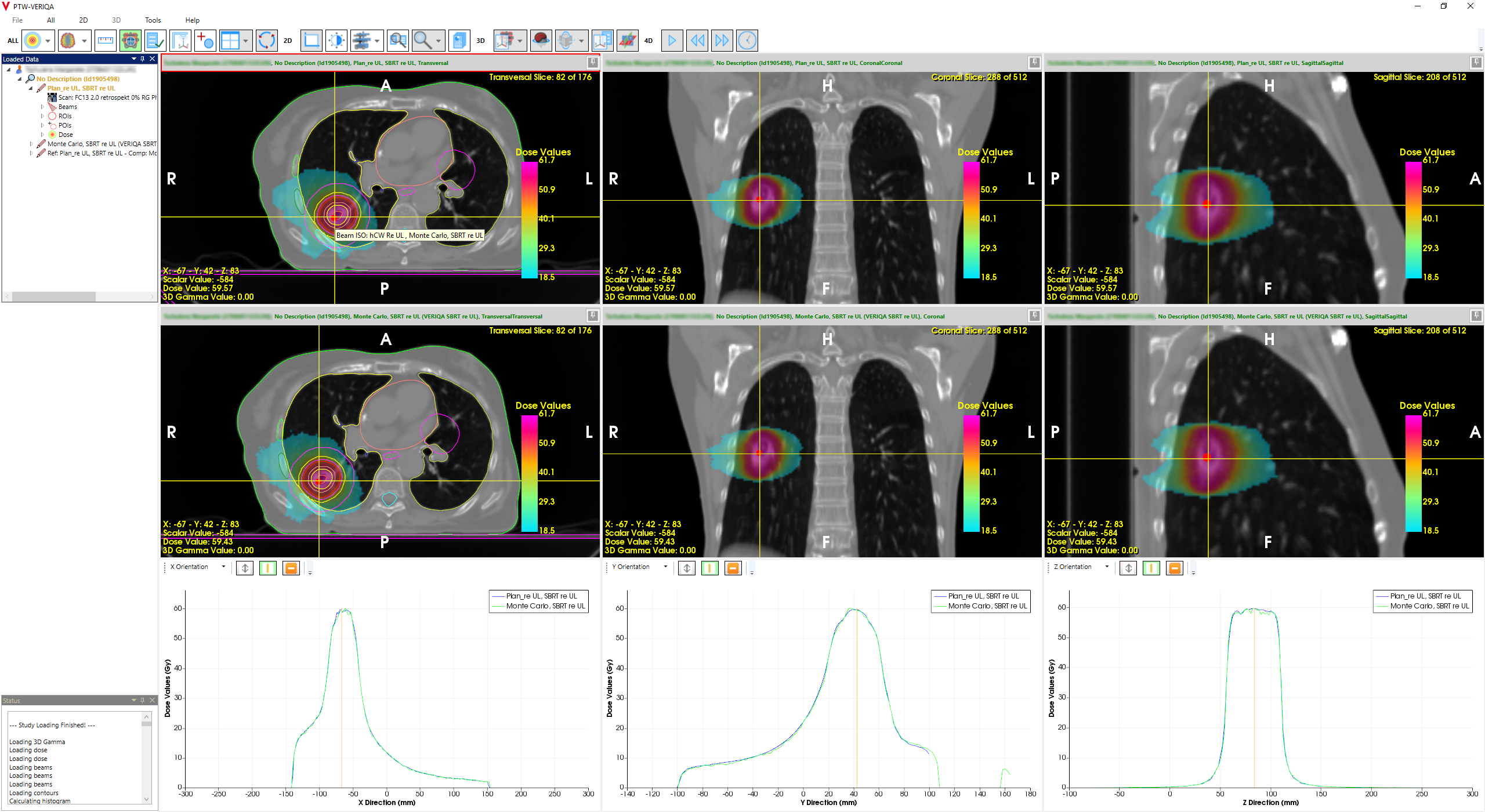
- Lung SBRT (8 x 6 Gy prescribed to the 80% isodose, 6FFF, AXB. GAI22 = 99.78%),
- VMAT of prostate + lymph nodes,
{kind=link}
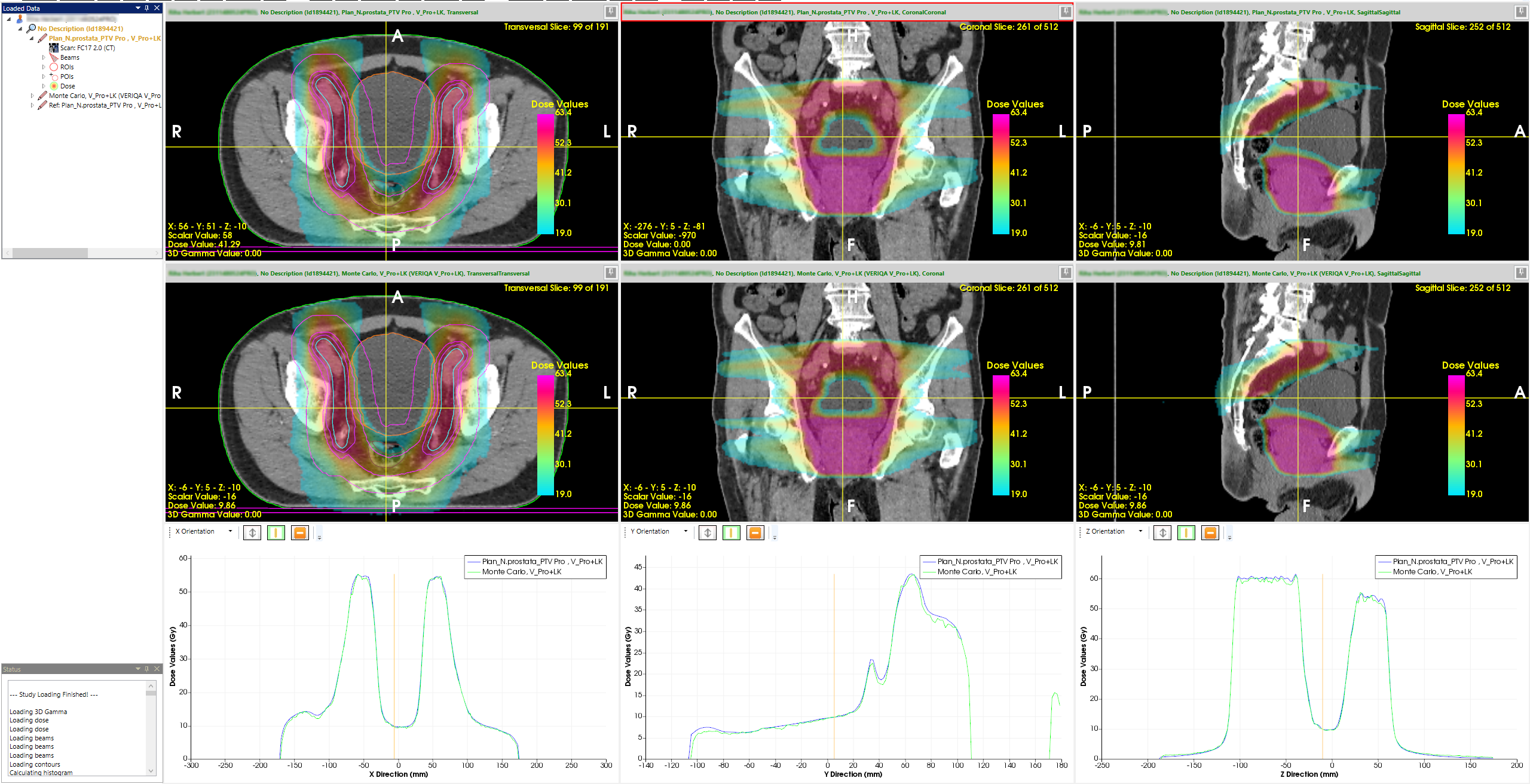
(VMAT PRO+LN, 10FFF, AAA. GAI22 = 99.81%)
- VMAT of prostate with double titanium hip implants,
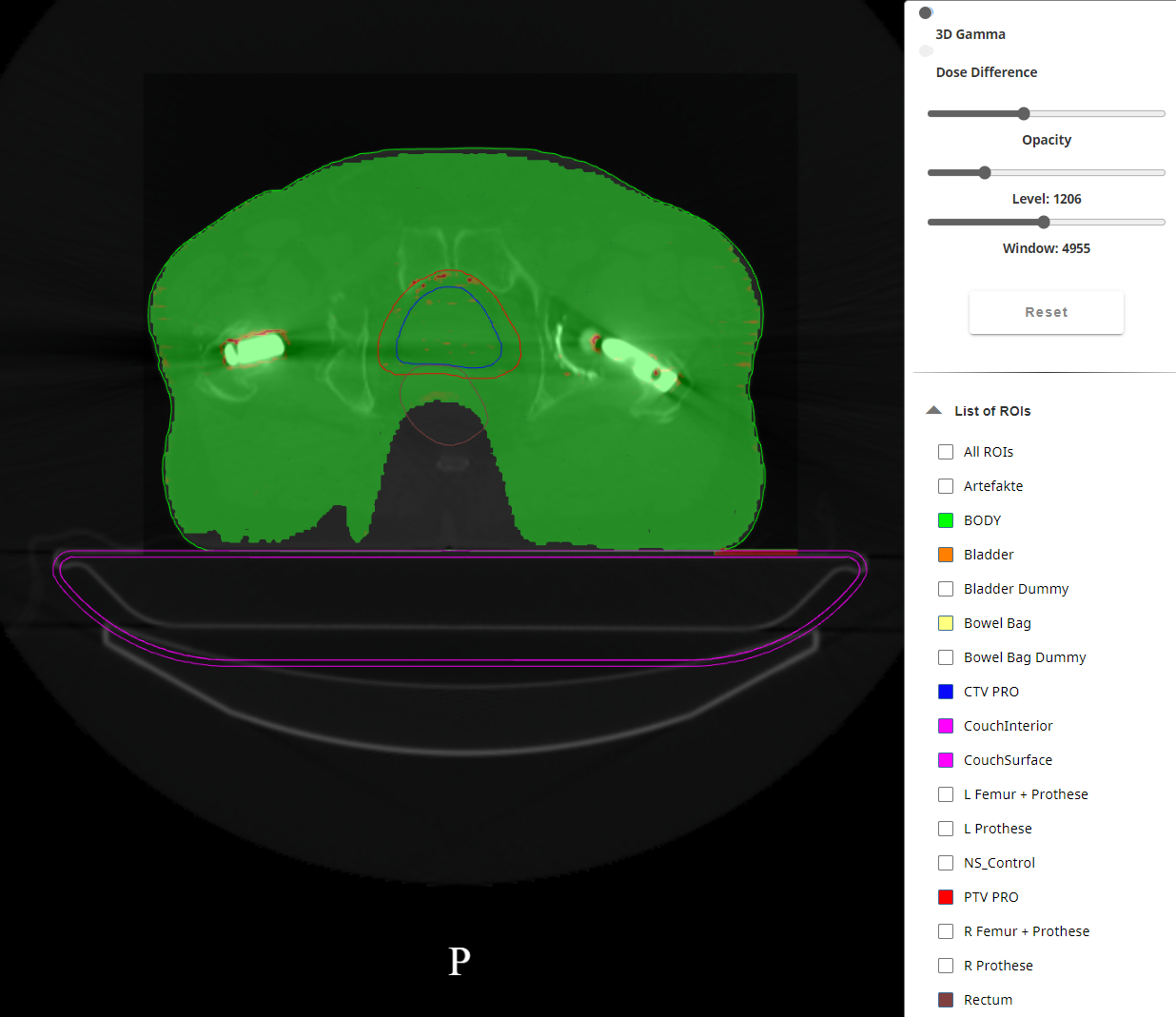
(Patient with double hip implants, 10FFF, AXB. GAI22 = 99.72%)
- HyperArc plan with 30 targets:
2.png)
(Note: This plan was not treated on a patient, but a patient CT dataset was used for planning.)
The last example, which has already been presented elsewhere, is not a clinical case but was designed to test the Eclipse's ability to handle such a large3 number of targets, and also to test the dosimetric verification chain.
In most clinical cases, i.e. when CT data is used, the match AXB/MC was better than AAA/MC. We had already observed this during preliminary testing. If AXB was the only TPS algorithm, it would probably be possible to use GAM22 as the default (which should "work" for most cases) for the VERIQA evaluations. However, since we use both AAA and AXB, we have to relax to the GAM33 test as default.
- 95.52% < GAI22 (clinical plans) < 99.98%
Conclusion
Due to the excellent results, VERIQA was accepted and commissioned for clinical use on July 04, 20244.
And now I see with eye serene
The very pulse of the machine.
(William Wordsworth, 1804)
Notes
1 The AXB algorithm requires material assignment if a structure is larger than 1.5 cm3.
2 The "Chair" is a remarkable DMLC test pattern which demonstrates several MLC features at once (static transmission, moving gap transmission, dose through wide and narrow gaps).
3 It may sound large, but in the case of inhomogeneous optimization, where several non-overlapping nested shell (helper) targets are sometimes used to concentrate dose in the center of each target, this number can be reached, although the number of clinical targets is much smaller.
4 One year later, on July 3, 2025, the Monte-Carlo calculation counter was close to 3000.
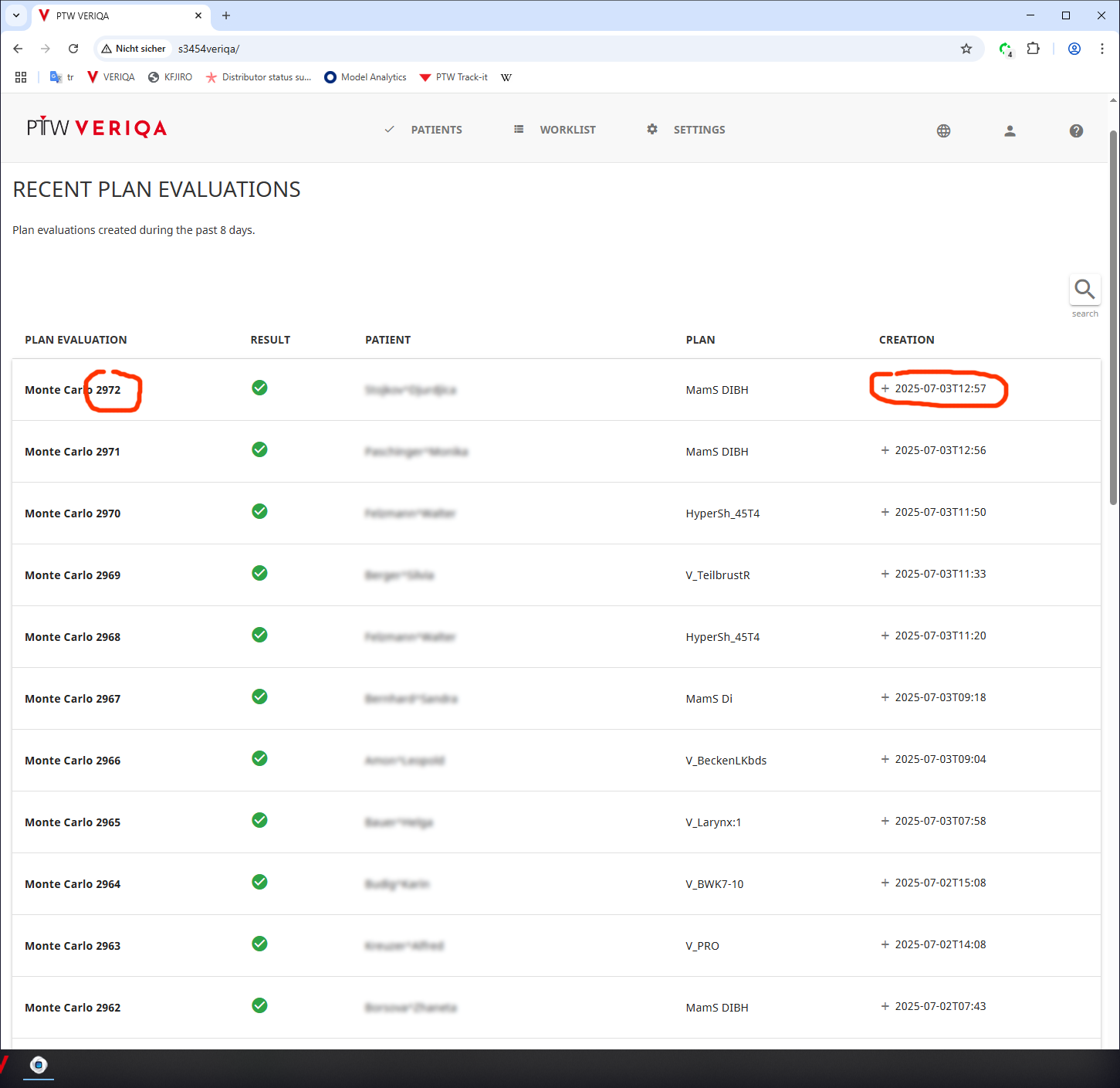{kind=link}