How we use the 2D-ARRAY for IMRT verification
Plan verification and field verification
There are two ways to verify an IMRT treatment plan: plan verification and field verification. For plan verification, the group of treatment fields is copied to a verification phantom in the TPS, preserving Gantry and Collimator angles. With this method, it is the superposition of the IMRT fields which is measured. With the 2D-ARRAY, a dose plane can be measured and compared to the TPS.
For field verification, a separate verification is done for every IMRT field. Beam incidence is orthogonal to the ARRAY surface. Collimator can either be set to zero, or the plan value. This is a matter of taste. However, the field is copied to the 3D-data set of the verification phantom in the same way as for the plan verification.
In either case, the clinical setup (buildup, SSD, isocenter position etc.) has to match the planned setup (Fig.1).
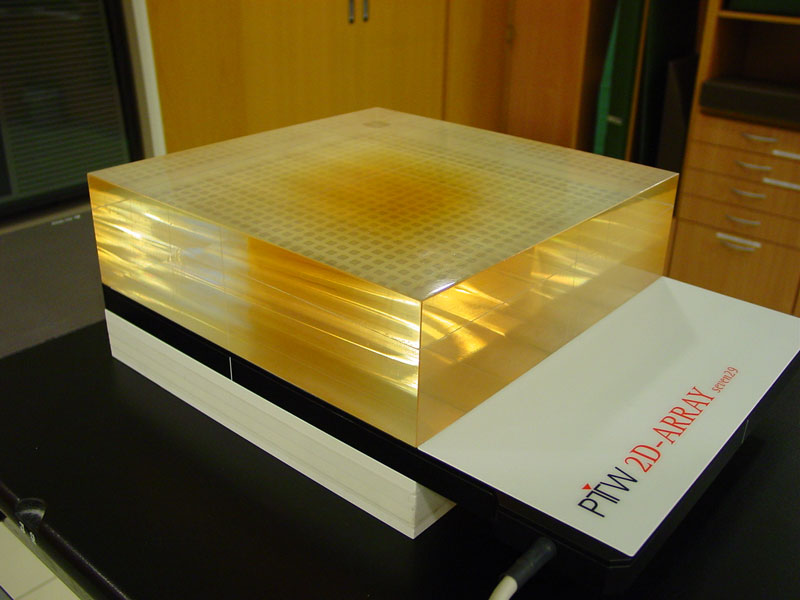
Fig.1: Typical setup for field or plan verification.
A dose plane is exported from the TPS, which corresponds to the measurement plane in the 2D-ARRAY. The planned and measured dose distributions are compared in VeriSoft (Fig.2):
Fig.2: Typical five field prostate plan with 15MV and Gantry angles 0°, 72°, 144°, 216°, 280°. For field verification, Gantry was always set to zero. Left: typical profile (blue: calculated, green: measured). Right: Gamma index, 3%, 3mm and isodose overlay. Field 1 (0°)
Field 2 (72°)
Field 3 (144°)
Field 4 (216°)
Field 5 (280°)
The same plan can be found here, verified with the aS500.
We use field verification in most cases, because the agreement can be checked for every single field. The plan verification is only used when the superposition is of special interest, e.g., when asymmetric non-IMRT fields and a group of IMRT fields share the same isocenter and should match at the field edge without major over- or underdosages (Fig.3).
Fig.3: Plan verification of five IMRT fields and one static supraclavicular field (click on images to enlarge). The abutting field edges at the central axis should be checked. The reasonable overdose at the central axis (+5.5% in the inplane profile) was considered to be clinically insignificant.
Plan verification aspects that should be considered:
- If the IMRT plan has both HiX (15MV) and LoX (6MV) fields like the example shown in Fig.3, on can only apply one single beam quality correction factor for both energies. The measurement cannot be stopped and a different correction factor applied.
- The 2D-ARRAY is not really water equivalent, just like RW-3 ("solid water") is not exactly water equivalent. However, when the beam enters at a very oblique angle, we saw that the degree of mismatch between TPS prediction and measurement depends more on the algorithm used in the TPS than on the water equivalence of the seven29: when using the new Anisotropic Analytical Algorithm (AAA) for dose calculation in Eclipse instead of the old Pencil Beam Convolution (PBC), the agreement was much better, even for beams entering at 95°.