Case Study: OCTAVIUS Verification of AAA and AXB SBRT plans
The findings of October 2013 shall be applied to a real lung stereotactic case, where two separate targets were treated with 10FFF, two half-arcs, using backup-gating. For the actual patient treatment,

(Fig 1: SBRT VMAT treatment of right lung, 13 Gy, TrueBeam 2.0, Perfect Pitch 6-DoF couch, backup gating.)
AAA plans were chosen. In this retrospective OCTAVIUS verification study, two AAA and Acuros XB (AXB) plans, similar to the clinically treated plans, shall be compared. Will AAA or AXB give better verification results with OCTAVIUS1?
Clinical Case
For the tumor in the left lung, the prescription to the PTV (67 ccm) is 15 Gy in 3 fractions:
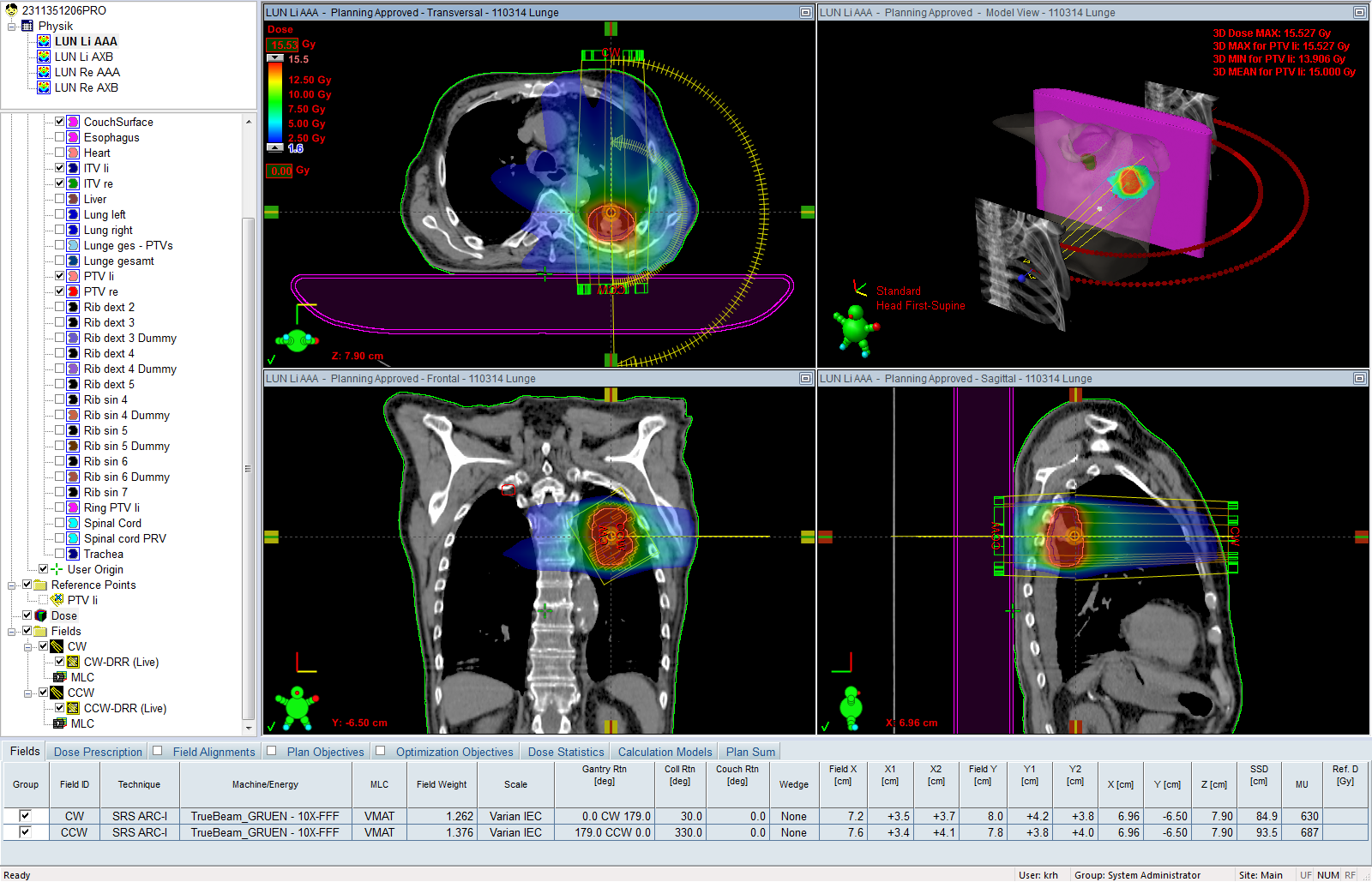
(Fig 2: SBRT VMAT plan of left lung, calculated with AAA version 11.0.31.)
In the same patient, a second PTV in the right lung (34 ccm) is planned to receive 39 Gy (3 times 13 Gy):
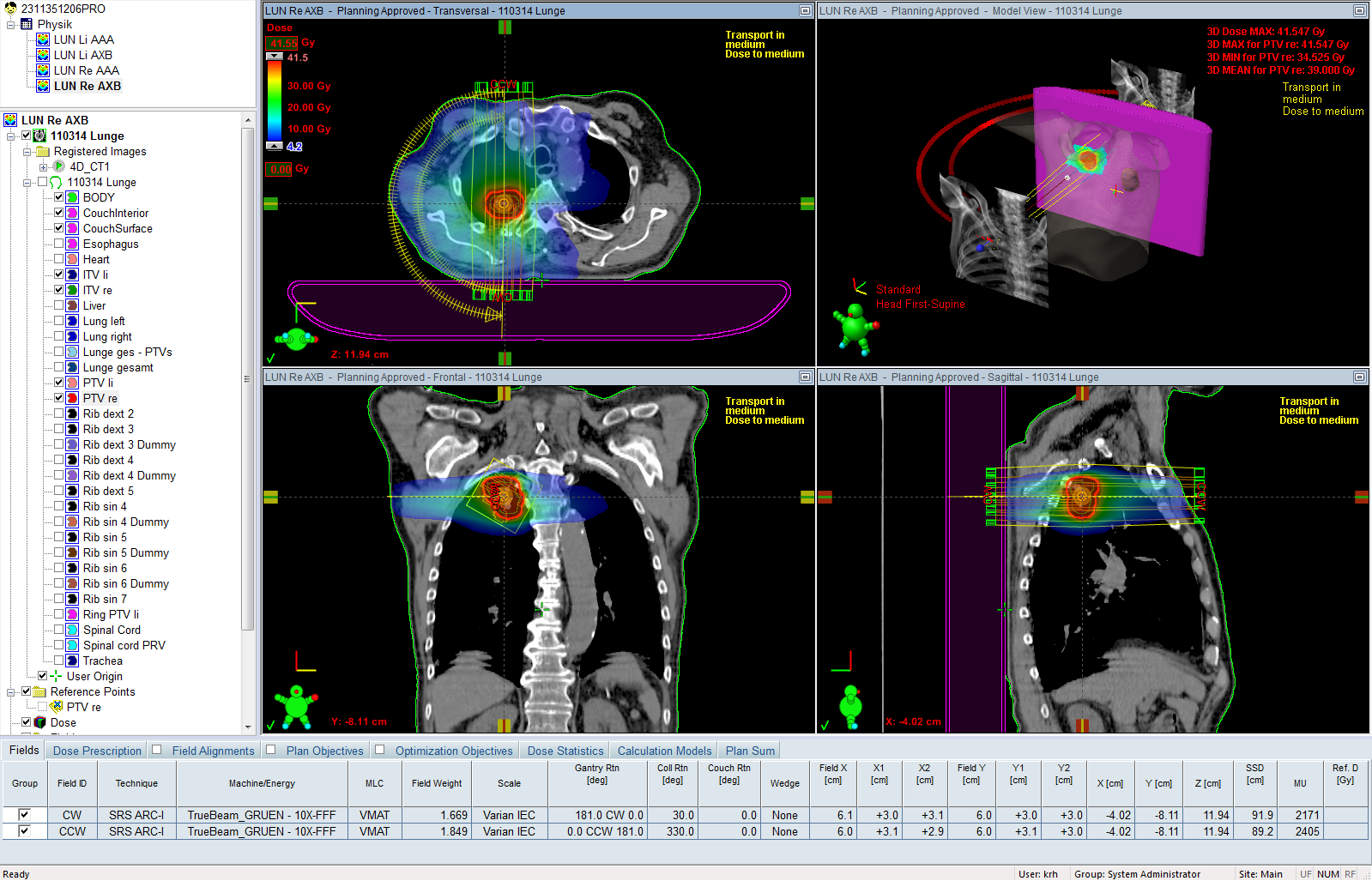
(Fig 3: SBRT VMAT plan of right lung, calculated with Acuros XB version 11.0.31.)
For this planning study, both targets were planned with both calculation algorithms. The plans were optimized with the Progressive Resolution Optimizer (PRO) version 11.0.31, using Intermediate Dose several times until no further improvement in plan quality was observed2. This is necessary for large inhomogeneities like the lung. All plans were dose normalized to target mean. Calculation grid size was 2.5 mm. For AXB plans, dose reporting mode was "Dose to medium".
OCTAVIUS Verification Plans
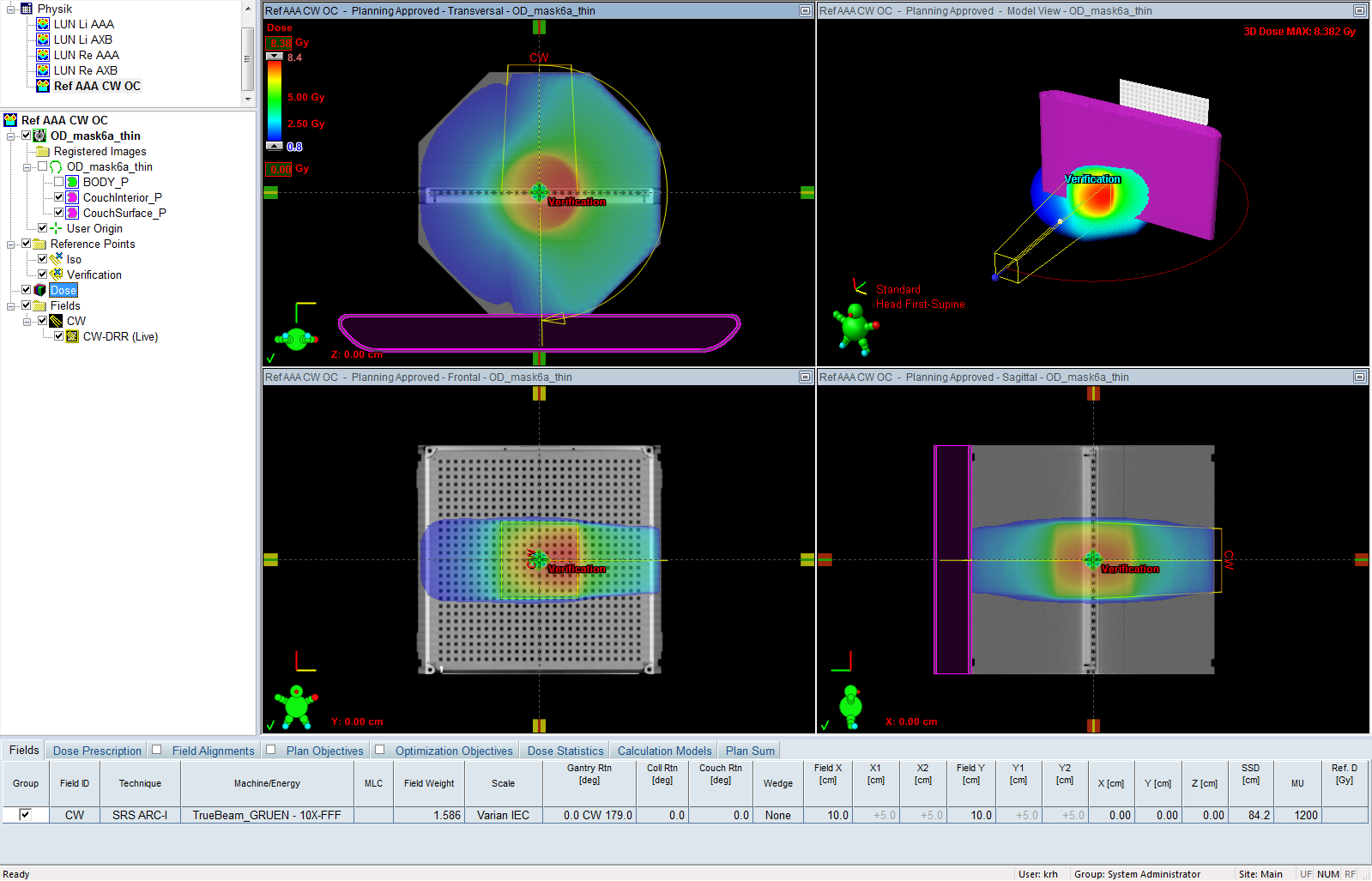
For the eight arcs (Left/right lung x CW/CCW x AAA/AXB = 8), verification plans were calculated on the PTW OCTAVIUS phantom (OP) using structure set "mask6a" and the thin Exact IGRT couch ("mask6a_thin").
As reference field for the determination of the cross-calibration factor kuser, we chose a static 10x10 half-arc on one side of the phantom. By comparing the CAX reference dose with the Eclipse reference dose, kuser was determined. Since the reference dose is depending on the selected algorithm, kuser will be different for AAA and AXB. In the structure set mask6a_thin, the material polystyrene was assigned to the whole BODY outline.
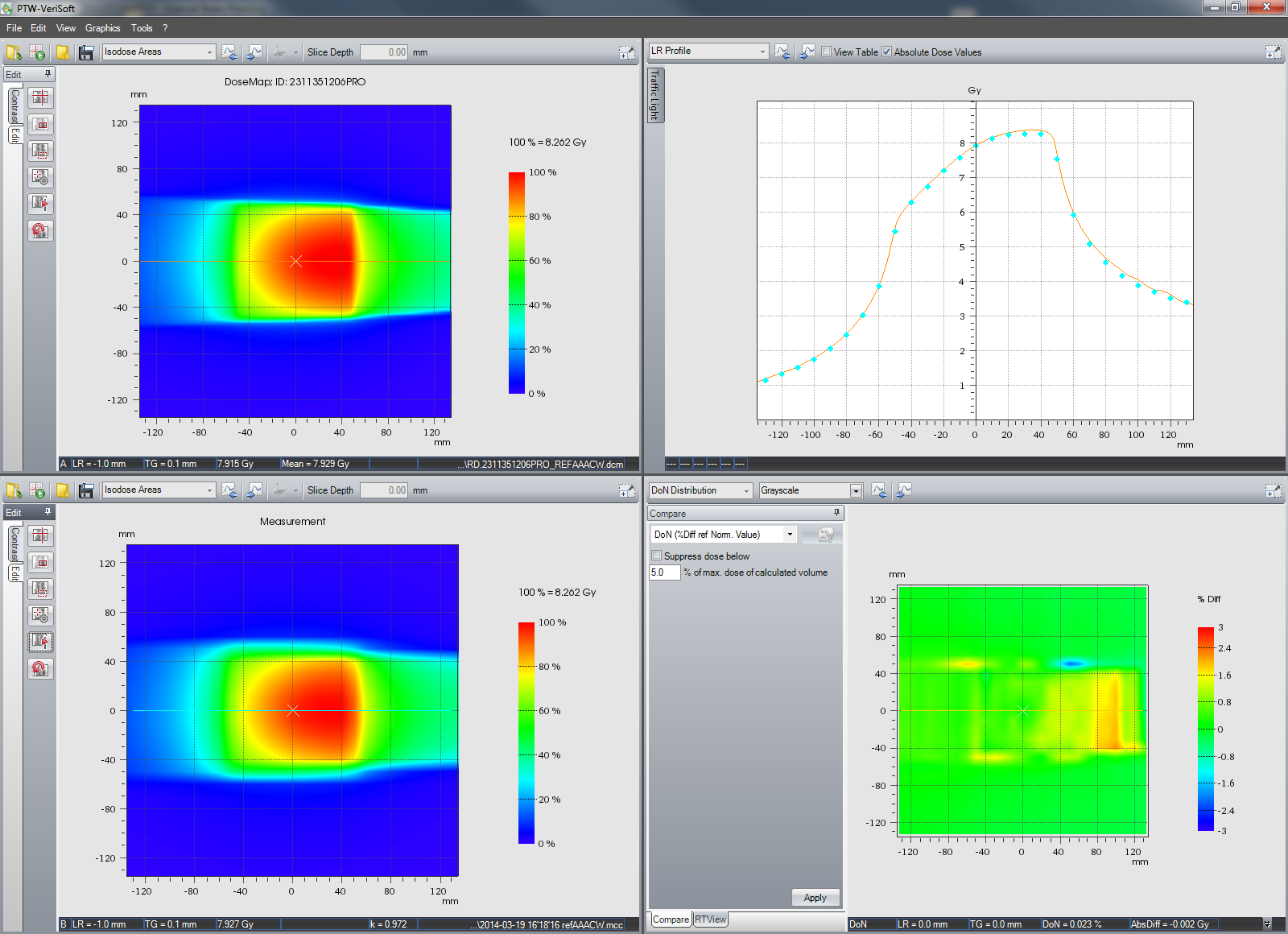
On the TrueBeam, the plans were measured with the PTW OCTAVIUS Detector 729 (OD) in horizontal orientation, and evaluated with VeriSoft 6.0. The 3%/3mm Gamma criterion was used, and the Gamma Agreement Index (GAI3,3 in percent) was determined.
{kind=link}
Results
Arcing over the right half of the OP gives an asymmetric dose distribution, which can nevertheless be cross-calibrated easily against the calculated matrix (C365 was used to determine kuser). This setup saves time during measurement. A full arc (360°) would not give any extra "information": the half arc already sees the influence of couchtop and the angular sensitivity dependence of the OD, and both will be "included" in the cross-calibration factor.
{kind=link}
{kind=link}
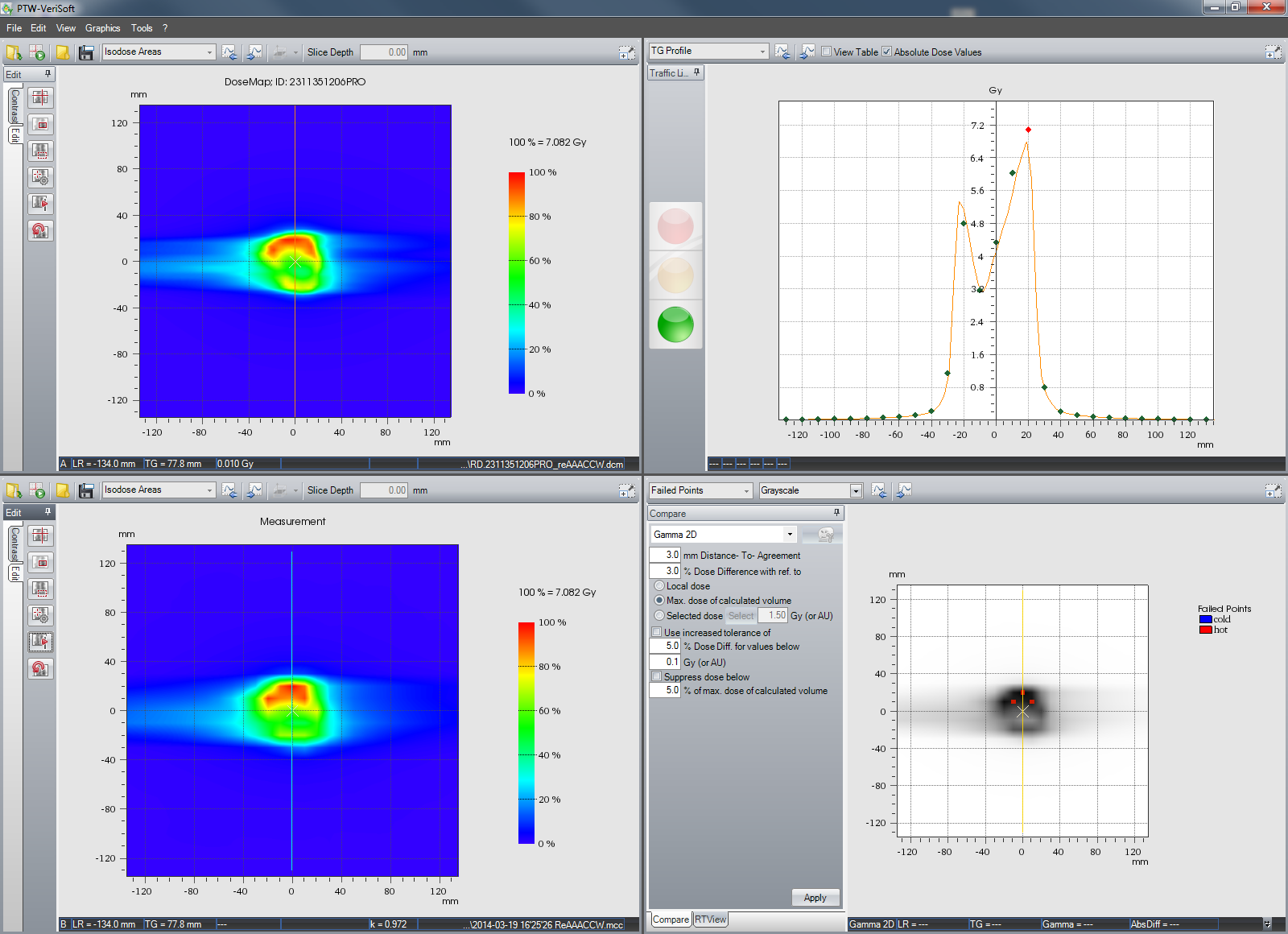
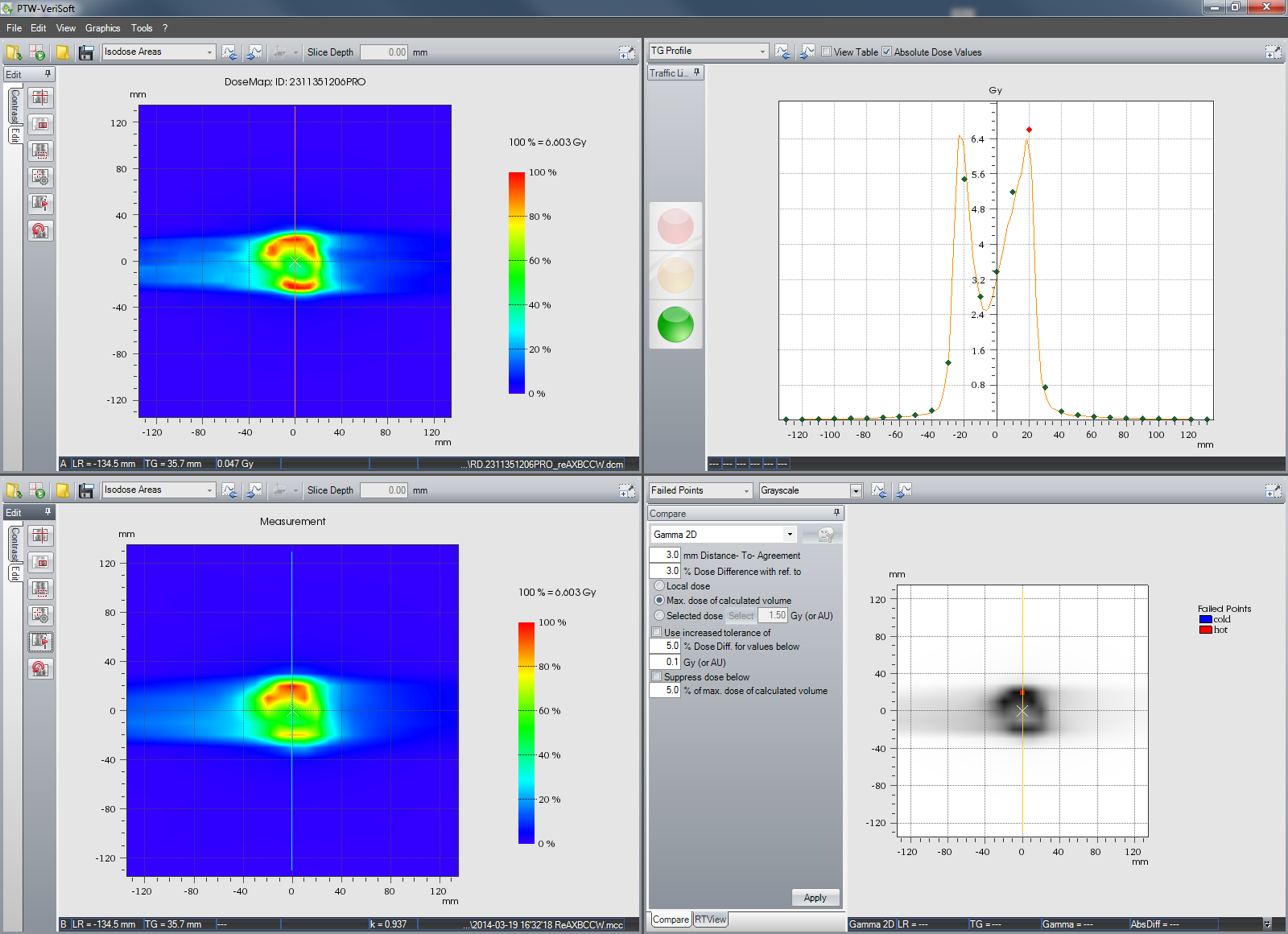
We found cross-calibration factors kuser(AAA) = 0.948 and kuser(AXB) = 0.914, which were successively applied to all plans calculated with the respective algorithms.
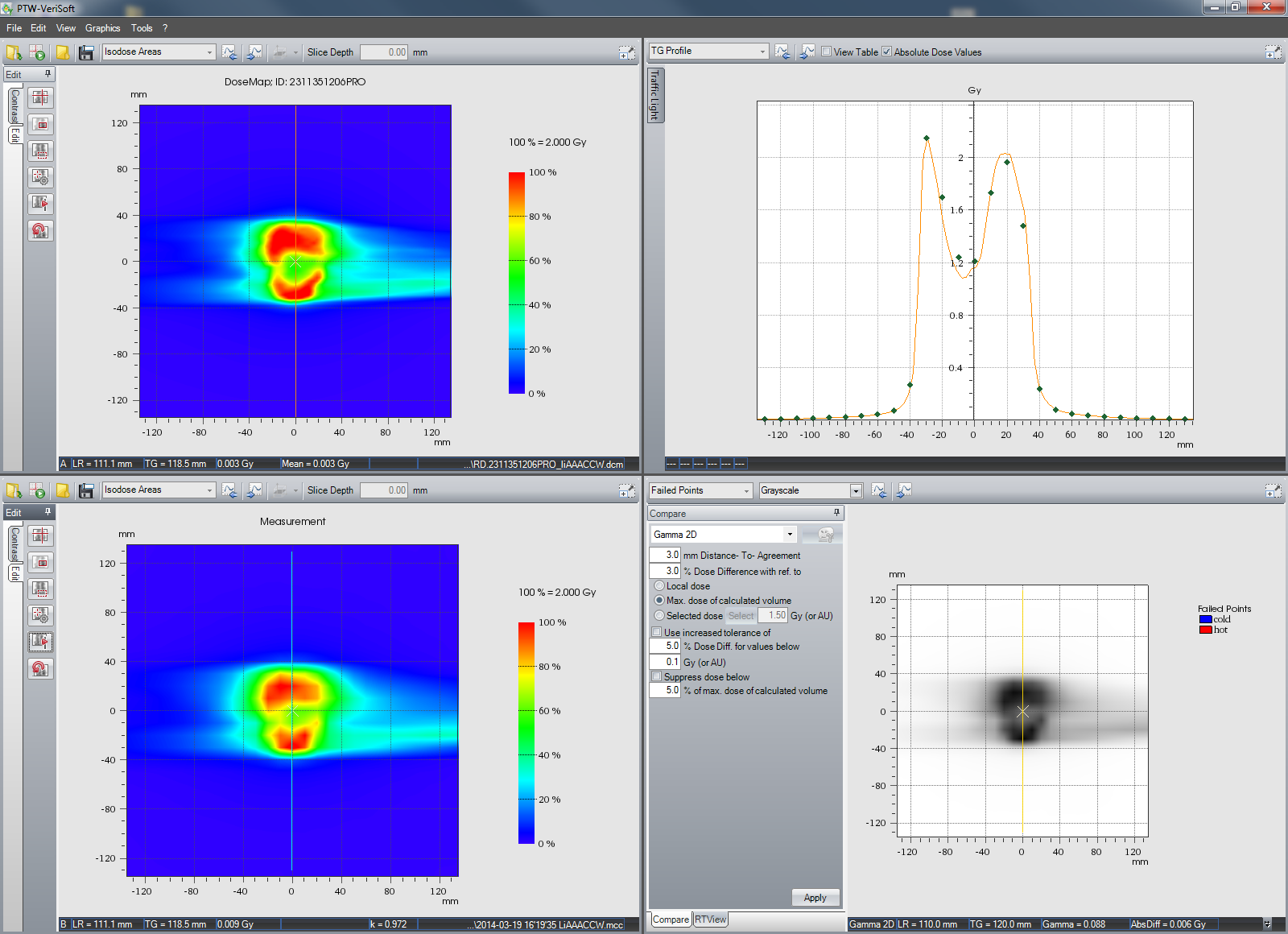
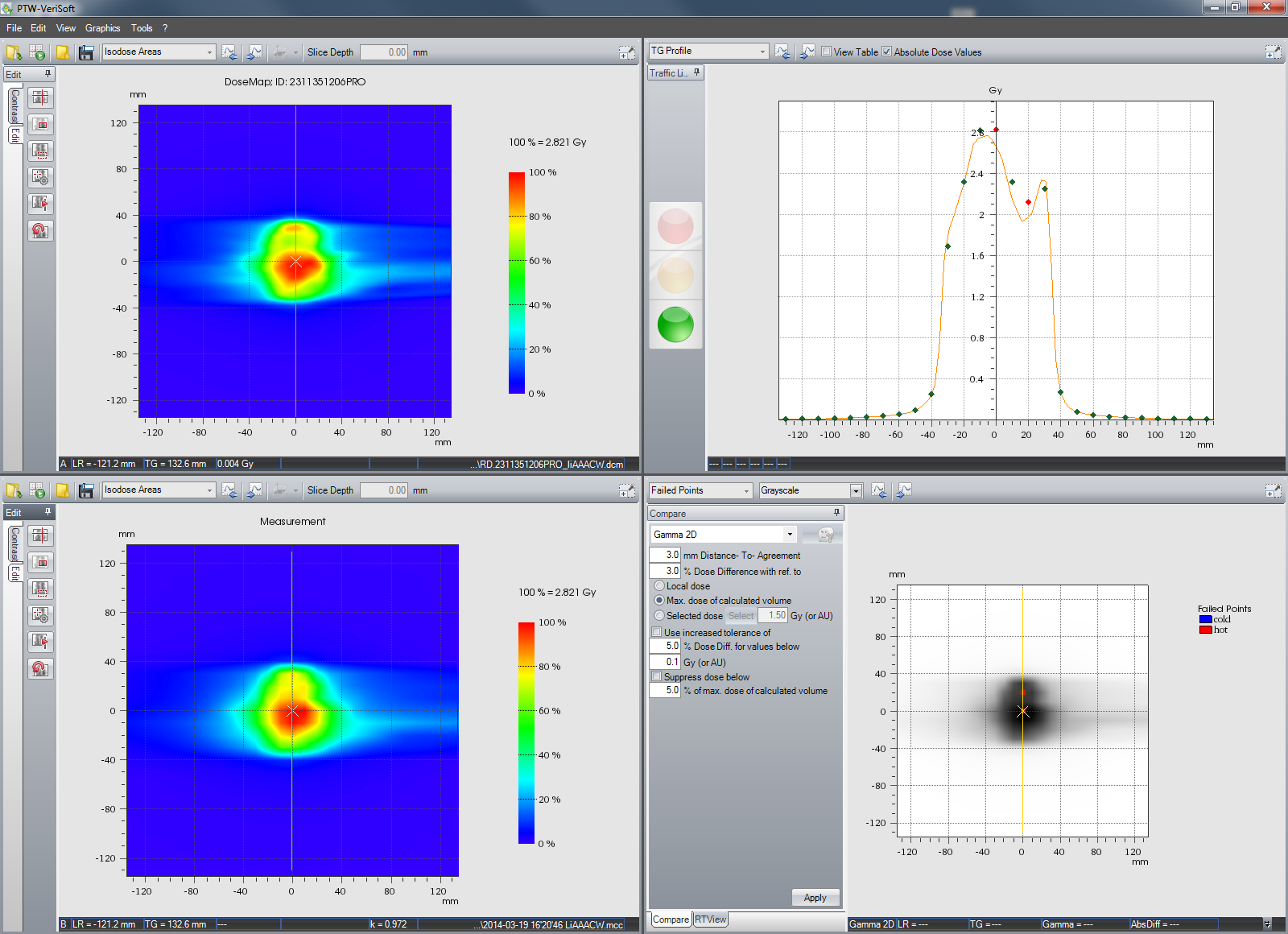
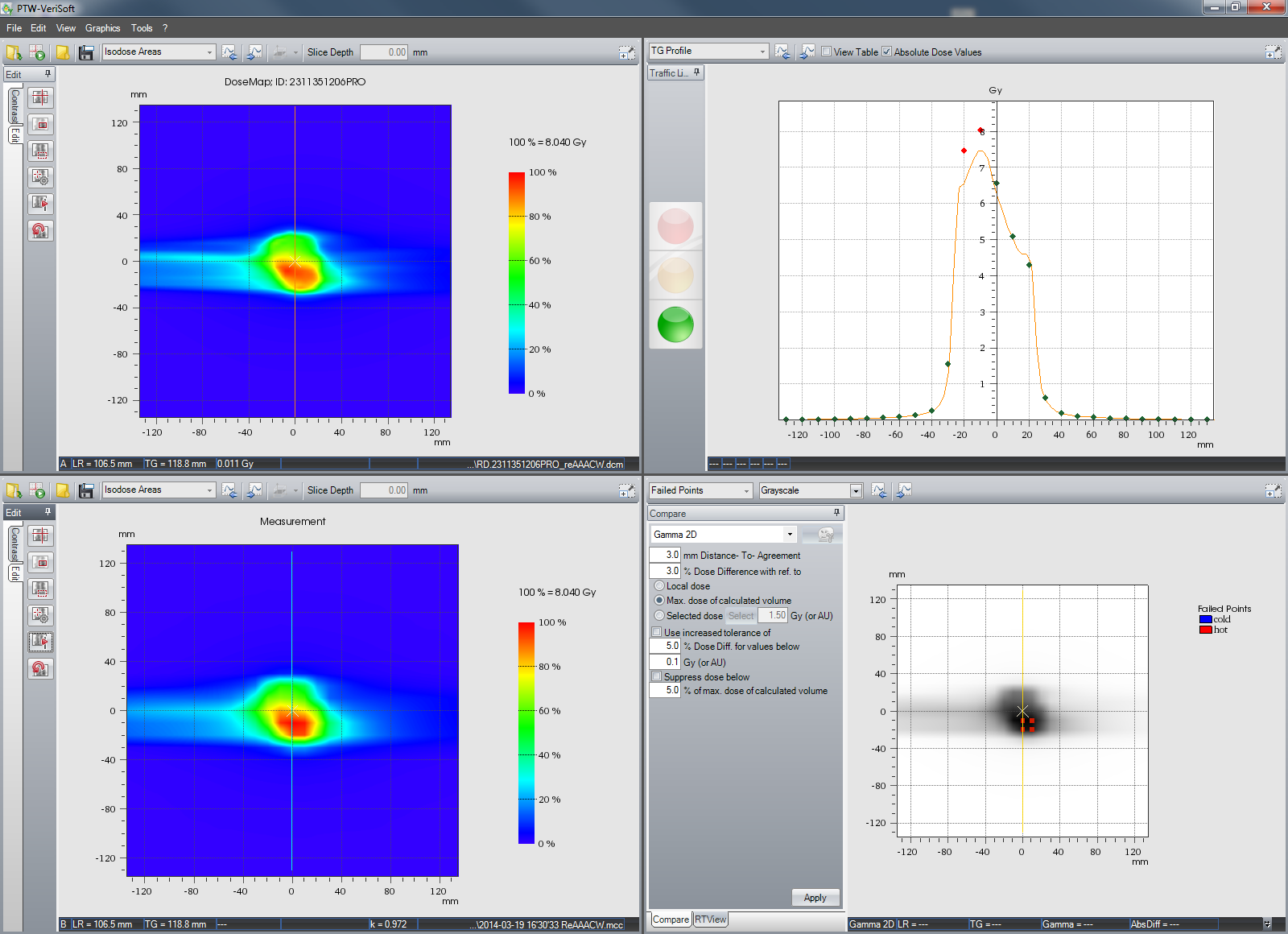
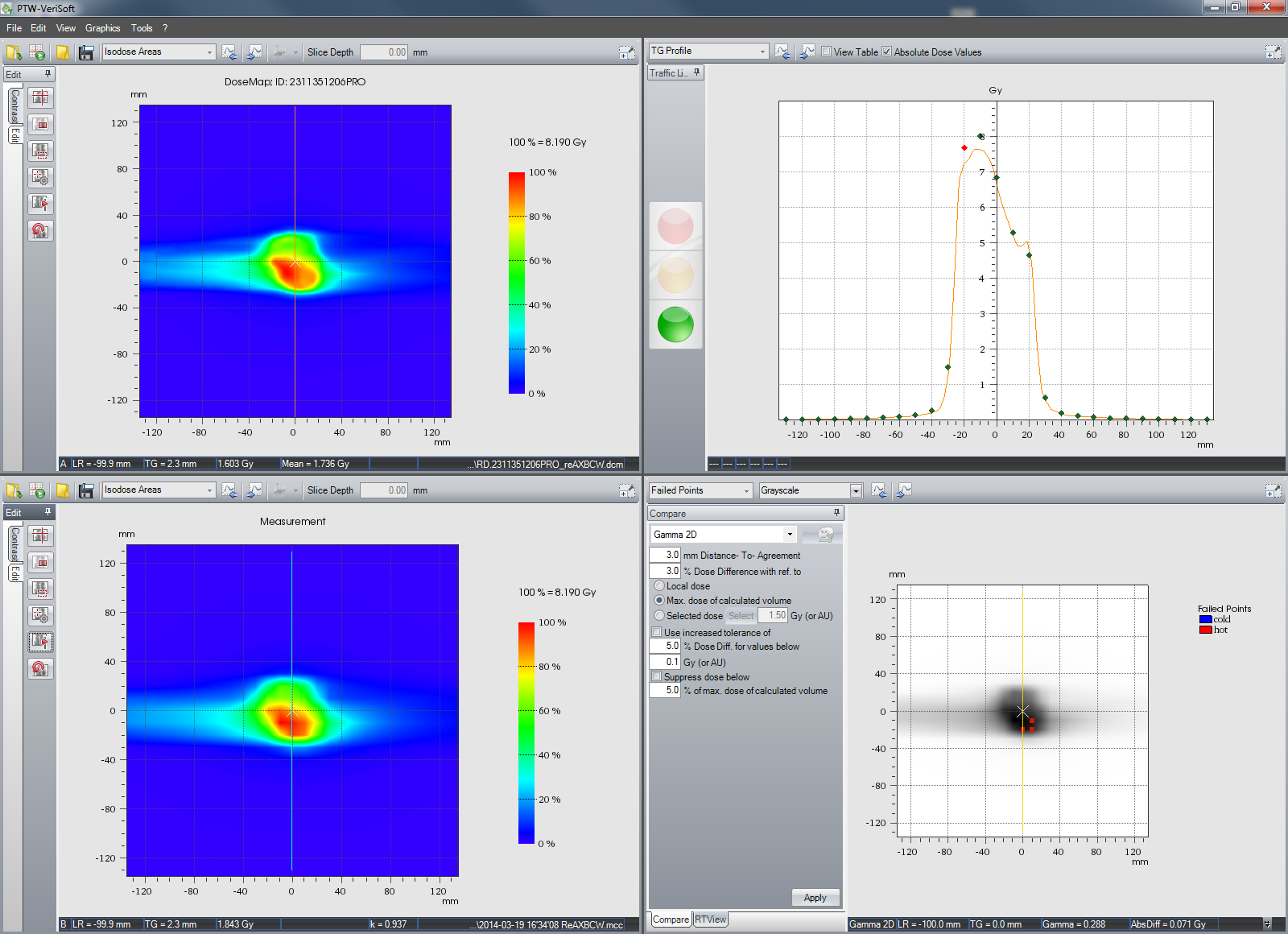
(Fig 4: VeriSoft evaluation of left lung, CCW arc, AAA.)
The OCTAVIUS verification results for the two calculation algorithms can be summed up as follows:
| AAA | AXB | ||||
|---|---|---|---|---|---|
| Target | Arc | GAI3,3[%] | Failed Points | GAI3,3[%] | Failed Points |
| PTV left lung | 0.0 CW 179.0 | 99.7 | 2 | 100.0 | - |
| PTV left lung | 179.0 CCW 0.0 | 100.0 | - | 100.0 | - |
| PTV right lung | 181.0 CW 0.0 | 99.5 | 4 | 99.6 | 3 |
| PTV right lung | 0.0 CCW 181.0 | 99.6 | 3 | 99.9 | 1 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Plans calculated with AXB gave slightly better OCTAVIUS verification results than plans calculated with AAA. Of course, one cannot generalize from a case study. However, the dosimetric verification of VMAT plans calculated with AXB is not "more challenging" than verifications of AAA plans.
Notes
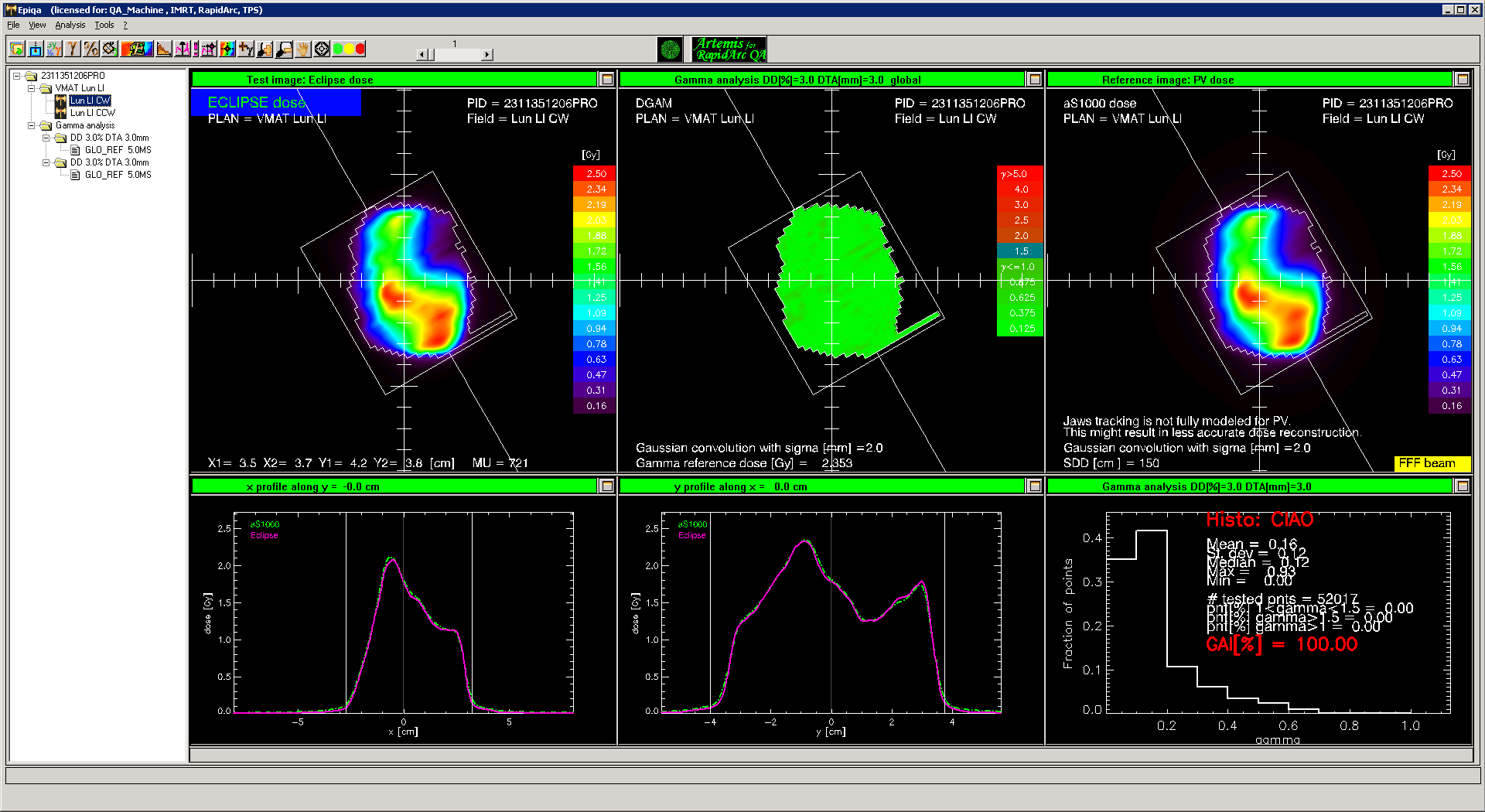
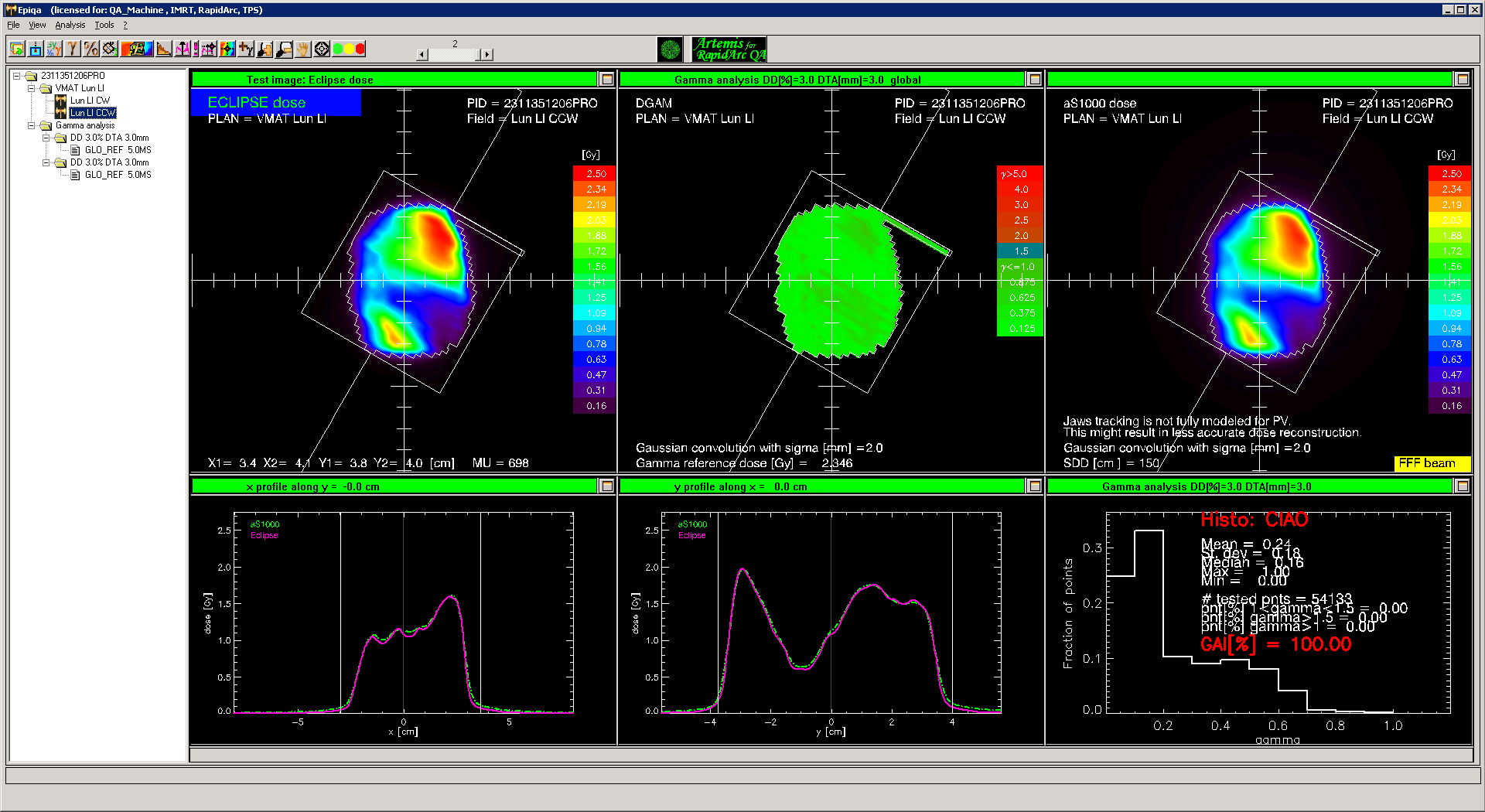
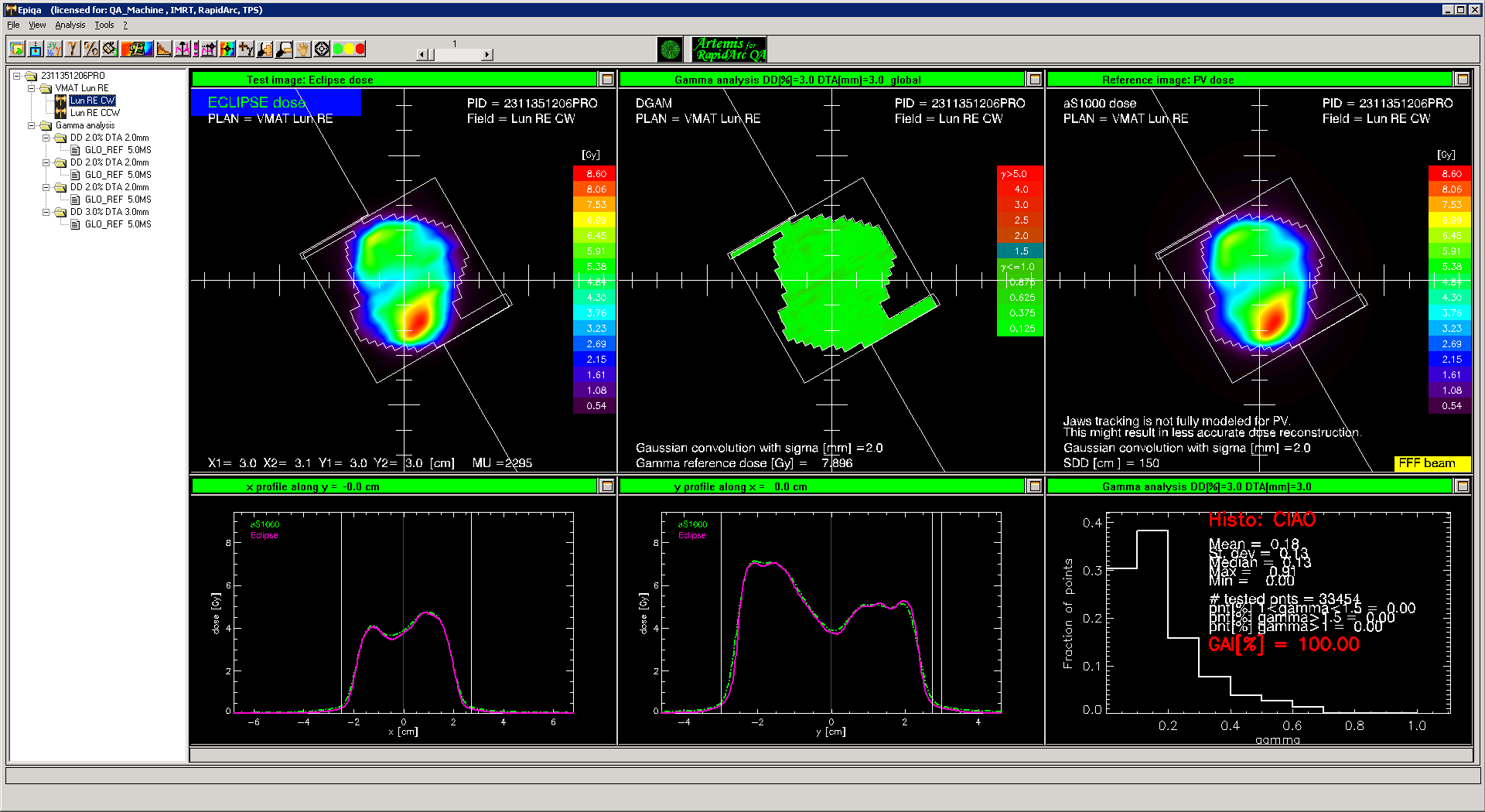
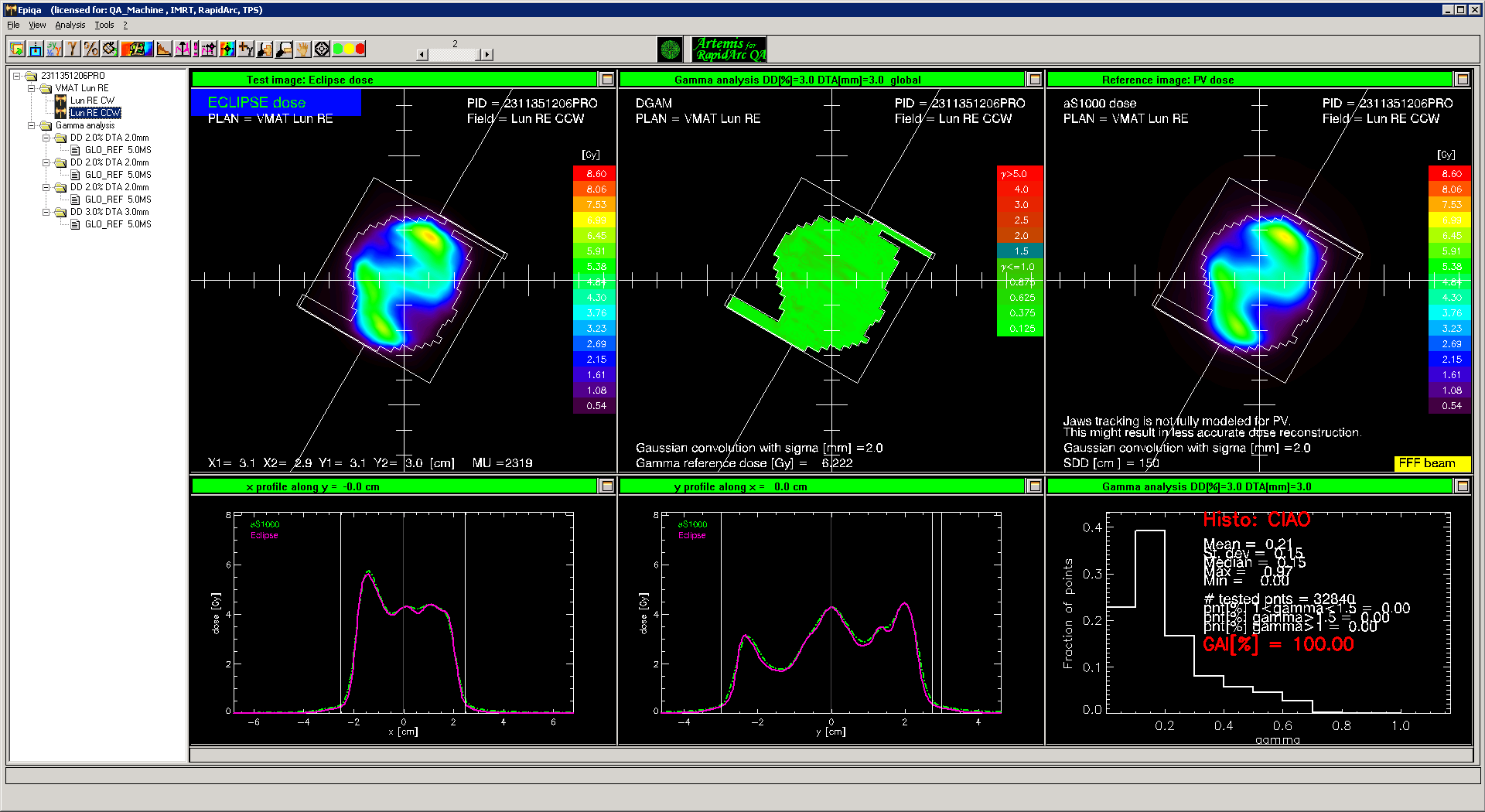
1The clinically treated arcs were verified with EPIQA 4.0.6, with the following results: LeftCW, LeftCCW, RightCW, RightCCW.
2The number of intermediate dose cycles needed for AXB is higher than for AAA.
{kind=link}
{kind=link}
{kind=link}
{kind=link}